서 론
비만 환자가 증가하면서 내시경 비만 치료 또는 비만 수술에 대한 관심이 매우 높다[1,2]. 현재 시행되고 있는 내시경 치료는 위풍선(intragastric balloon) 삽입술, 위성형술(gastroplasty), 흡입 치료(aspiration therapy) 등이 있다[3]. 이 중 가장 먼저 시작된 방법은 위풍선 삽입술로[4], 현재 미국이나 유럽에서 활발하게 시행되고 있고 단기간의 체중 감량 효과가 입증되었다[4-7].
최근 국내에서도 내시경을 통한 위풍선 삽입술의 시행 횟수가 점차 증가하고 있으나[8,9] 위풍선을 제거한 후에도 감소된 체중이 유지되는지는 명확하지 않고, 관련된 연구 역시 부족하다[10]. 현재 내시경 비만 치료는 체질량지수(BMI)가 35 kg/m2 이상이거나 체질량지수가 30 kg/m2 이상이면서 이상지질혈증(dyslipidemia), 2형 당뇨, 고혈압 등의 대사성 질환이 동반된 사람들에게 우선 권고되고 있다[2,8]. 그러나 실제로는 단순히 미용 목적으로 시행되는 경우가 많고, 시술에 따른 합병증에 대한 고려가 충분히 이루어지지 않아 문제가 되고 있다.
본원에서는 생활습관 변경(lifestyle modification)이나 약물 치료(pharmacotherapy)에 실패한 12명의 환자에게 지난 4년 동안 위풍선 삽입술을 시행하였고, 그중 11명을 6개월간 추적 관찰하였다. 본고에서는 위풍선 삽입술의 단기 치료 결과와 동반된 합병증을 보고하고자 한다.
증 례
2016년에서 2019년 사이에 내시경 비만 치료를 위하여 본원에 내원한 사람은 총 12명이었다. 이들은 이전에 식이 조절이나 운동 요법, 약물 치료에 실패하였고, 수술 치료에 대한 두려움과 거부감을 가지고 있었다. 상부위장관 수술력이나 악성 종양의 과거력이 있던 사람은 없었다. 12명의 환자에게 위풍선을 삽입하였으나 1명은 하루 만에 제거하여 추적 관찰은 나머지 11명을 대상으로 이루어졌다. 이 증례 보고는 위풍선 삽입술의 단기 체중 감량 효과를 정량적으로 분석하고, 대사성 질환과 관련된 지표들의 변화 양상 및 시술에 동반된 합병증을 알아보고자 하였다.
체중 감량 효과를 확인하기 위하여 체중, 체질량지수, 총 체중 감량률(total body weight loss, %), 초과 체중 감량률(excess weight loss, %)을 계산하여 비교하였다. 체질량지수는 체중(kg)을 키(m)의 제곱으로 나눈 값으로, 우리나라의 비만 기준은 체질량지수 25 kg/m2 이상이다. 총 체중 감량률은 시술 전의 체중에 대하여 시술 후에 얼마나 감량하였는지를 비율로 나타낸 것이고, 초과 체중 감량률은 체질량지수 25 kg/m2 기준으로 초과된 체중에서 얼마나 감량하였는지를 보여주는 것이다[4].
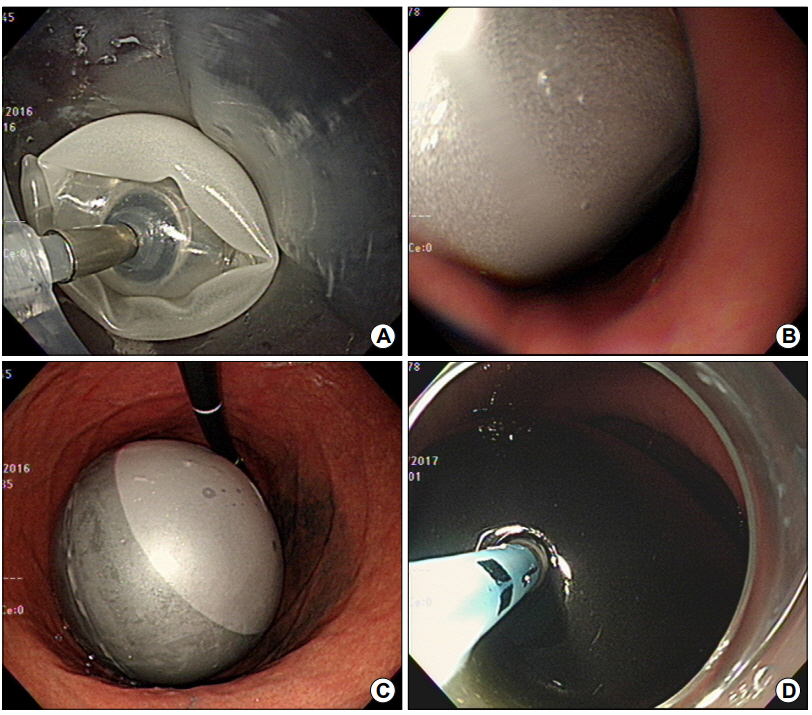
11명의 환자들은 시술 당일, 시술 1개월, 2개월, 6개월 후에 내원하여 체중을 측정하였고, 불편한 증상을 보고하였다. 위풍선 삽입일과 그로부터 6개월 후인 위풍선 제거일에는 추가로 혈압을 측정하고 혈액 검사를 시행하였다. 시술은 내시경을 통하여 위 안에 엔드볼(End-Ball®; Endalis, Brignais, France)이라는 풍선을 삽입하고 400~600 mL의 공기와 생리식염수를 풍선 안에 넣어 부풀리는 방식으로 진행되었다(Fig. 1).
위풍선 삽입 후 6개월간 추적 관찰을 완료한 11명의 평균 나이는 40.1±14.4세였고, 이 중에서 여자는 9명이었다(Table 1). 이전에 체중 감량을 위하여 약물을 복용하였던 환자는 6명이었다. 시술 당일 평균 체중은 85.6±10.7 kg, 평균 체질량지수는 32.0±3.7 kg/m2였고, 체질량지수가 35 kg/m2 이상인 사람은 4명이었다. 동반된 질환으로는 고혈압과 당뇨가 가장 많았고 대사 증후군(metabolic syndrome)에 해당하는 사람도 3명이 있었다. 대사 증후군이란 심혈관 질환에 대한 위험 요인들과 관련된 용어로, 1) 복부 비만(허리둘레 ≥102 cm [남], ≥88 cm [여]), 2) 혈청 중성지방 ≥150 mg/dL, 3) 혈청 고밀도지질단백(HDL) 콜레스테롤 <40 mg/dL (남), <50 mg/dL (여), 4) 혈압 ≥130/85 mmHg, 5) 공복 혈당 ≥110 mg/dL 또는 당뇨, 이 중 3가지 이상을 만족할 때로 정의한다[11].
위풍선을 6개월간 유치한 후 체중은 8.9±5.4 kg, 체질량지수는 3.3±2.0 kg/m2만큼 감소하였고 이는 모두 통계적으로 유의하였다(both P<0.001) (Table 2). 저밀도지질단백(LDL) 콜레스테롤의 경우 18.0±18.2 mg/dL만큼의 감량 효과가 있었다(P=0.027). 혈압과 혈당, 총 콜레스테롤, 중성지방, HDL 콜레스테롤도 6개월 후 수치는 낮아졌으나 통계적으로 유의하지는 않았다.
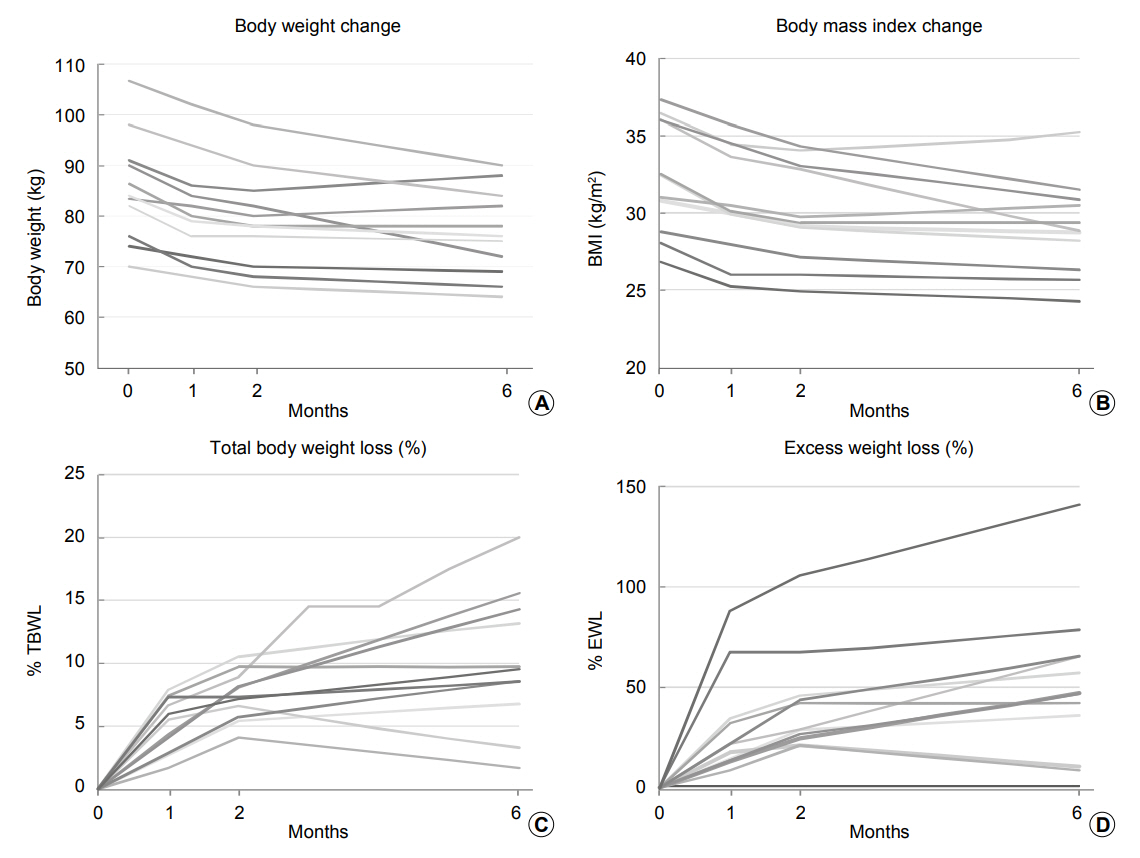
체중 감량의 추세는 0, 1, 2, 6개월 후의 체중, 체질량지수, 총 체중 감량률, 초과 체중 감량률의 변화로 확인하였다(Table 3). 총 체중 감량률은 평균 10.1±5.4%, 초과 체중 감량률은 평균 54.4±36.0%를 보였다. 치료에 대한 반응을 6개월 후 총 체중 감량률이 5% 이상일 때로 정의하였을 때[12], 11명 중 9명에서 치료에 대한 반응이 있었다. 1, 2, 6개월 후의 체중 변화 추세를 보면(Fig. 2), 특히 시술 직후 1개월 이내에 체중 감량 효과가 큰 것을 확인할 수 있었다.
위풍선 삽입술 후 가장 흔한 부작용은 구역감과 명치부 통증이었다. 시술 하루 만에 풍선을 제거한 환자가 있었는데, 기저질환이 없는 54세 여성이었다. 이 환자는 위풍선을 삽입한 직후부터 구역감, 구토, 심한 복통을 호소하여 영상학적 검사 및 혈액 검사를 추가로 시행하였고, 검사 결과 천공이나 장폐색 등의 심각한 합병증은 없었다. 그러나 환자 본인이 주관적으로 느끼는 통증의 정도가 심하여 더 이상 치료를 유지할 수 없었다.
6개월간의 추적 검사를 완료한 나머지 11명의 환자 중 10명에서도 시술 직후 구역감, 복통 등의 합병증이 있었으나 경미한 수준이었고 1~2주 안에 호전되었다. 11명 중 6명은 추적이 끊긴 상태이고, 5명은 이후 병원에 내원하였다. 이들 중 일부는 위풍선 제거 후 근소하게 체중이 증가하여 다시 삽입하기를 희망하였고, 실제로 1명은 풍선 제거 1년 후 두 번째 위풍선을 삽입하였다.
고 찰
본 증례 보고는 내시경 비만 치료를 위하여 내원한 11명의 환자에게 위풍선을 삽입하고 6개월간 추적 관찰을 시행한 치료 결과에 대한 것이다. 위풍선 삽입술 후 총 체중 감량률은 평균 10.1%, 초과 체중 감량률은 평균 54.4%를 보여주어 단기간의 체중 감량 효과를 확인할 수 있었다. 그러나 대사성 질환 자체가 개선되는 것은 이번 연구에서 입증되지 않았다[3,4,6,9]. 위풍선을 삽입한 12명의 환자 중 1명은 복부 불편감으로 조기에 풍선을 제거하였으며, 나머지 11명에서는 심각한 부작용이 발생하지 않았다.
현재 시행되고 있는 내시경 비만 치료는 위풍선 삽입술, 위성형술, 흡입 치료, 십이지장-공장 우회소매(duodenal-jejunal bypass liner), 내시경 위축소술(endoscopic gastric plication), 일차 내시경 비만 수술(primary obesity surgery endoluminal procedure) 등이 있다[5]. 내시경 비만 치료의 원리는 위 용적을 줄이거나 영양분의 흡수를 줄이는 것인데, 이 중 미국 식품의약국(Food and Drug Administration)의 승인을 받은 방법은 위풍선 삽입술, 위성형술, 흡입 치료이다. 위풍선 삽입술은 조기에 포만감을 주고 위배출(gastric emptying)을 지연시켜 식사량이 줄면서 체중도 줄어든다. 또한 그렐린(ghrelin), 렙틴(leptin) 등의 다양한 신경호르몬의 작용에도 영향을 준다고 알려져 있다[8,10].
최근 시행된 메타분석에서[5] 내시경 비만 치료를 받은 환자들은 생활습관만 조절하는 환자들과 비교하였을 때 6개월 후 총 체중 감량률과 초과 체중 감량률이 유의하게 감소하는 것으로 나타났다. 액체주입풍선(fluid-filled balloon)의 경우 대조군에 비하여 5.3%의 총 체중 감량률, 22.4%의 초과 체중 감량률을 보여주었다. 위풍선 삽입 후 12개월까지 추적하여 감량된 체중이 유지된 연구 결과도 있다(REDUCE Pivotal Trial) [7]. 이 연구에서 위풍선을 삽입한 환자는 체중 감량뿐만 아니라 삶의 질도 개선되었다고 보고하였다.
비만은 단순히 외형적인 문제일 뿐 아니라 2형 당뇨나 고혈압, 이상지질혈증, 심혈관 질환 등과도 연관이 있으며[13,14], 악성 종양의 발생에 영향을 미친다는 연구들도 보고되고 있다[1,12,15,16]. 위풍선 삽입은 체중 감량과 더불어 이러한 비만과 관련된 질환들이 호전되는 결과를 기대할 수 있어[13], 고도 비만의 경우에는 적극적인 치료가 필요하다.
국내에서도 내시경 비만 치료 시술이 많이 시행되는 것으로 추정되나 그 효과에 대한 연구 보고는 현재까지 없다. 이번 연구는 위풍선 삽입술 후 단기간의 체중 감량 효과와 안전성을 보여준 국내의 첫 번째 연구로 의의가 있다. 또한 12명 중 위풍선을 6개월 동안 유지한 사람이 11명에 달하여 높은 치료 순응도를 보여주었고, 심각한 합병증은 한 차례도 발생하지 않았다. 그러나 시술을 받은 환자수가 11명으로 적었고, 2명은 총 체중 감량률이 5% 미만이므로 어떠한 환자에서 위풍선 치료가 더 효과적일지에 대해서는 추가 연구가 필요할 것으로 보인다. 시술 6개월 후 환자의 콜레스테롤, 공복 혈당, 혈압 등에서는 의미 있는 호전을 보이지 않았지만 이것은 적은 환자수와 짧은 추적 관찰 기간 때문일 수 있다.
요약하면, 비만 치료를 위하여 11명에게 삽입한 위풍선은 단기간의 유의한 체중 감량 효과를 보여주었다. 그러나 장기적으로 체중 감량 효과가 유지되는지와 대사성 질환과 관련된 지표들이 호전되는지에 대해서는 추가적인 연구가 필요할 것으로 보인다. 위풍선 삽입술을 포함한 내시경 비만 치료들이 효과적으로 시행되기 위해서는 적절한 대상자의 범위와 시술 합병증에 대한 대처가 앞으로 해결해야 할 과제일 것이다.