ņä£ ļĪĀ
ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼(Helicobacter pylori, H. pylori) ņĀ£ĻĘĀņØĆ ĻČżņ¢æ ņ╣śļŻīļź╝ Ē¢źņāüņŗ£ĒéżĻ│Ā ĻČżņ¢æņØś ņ×¼ļ░£ņØä Ļ░Éņåīņŗ£Ēé©ļŗż. ļśÉĒĢ£ ņ£äņĢöņØś ņśłļ░® ĒÜ©Ļ│╝ņÖĆ ņĢäņÜĖļ¤¼ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØś ņøÉņØĖņ£╝ļĪ£ņä£ Ļ░ÉņŚ╝ņŚÉ ļīĆĒĢ£ Ļ▓Ćņé¼ņÖĆ ņĀ£ĻĘĀņØä ņØ╝ņ░©ņĀüņ£╝ļĪ£ ņČöņ▓£ĒĢśĻ│Ā ņ׳ļŗż[1,2]. ĻĄŁļé┤ņØś Ļ▓ĮņÜ░ņŚÉņä£ļÅä 2018ļģä 1ņøö ņØ┤Ēøä H. pylori ņĀ£ĻĘĀņŚÉ ļīĆĒĢ£ ļ│┤ĒŚśĻĖēņŚ¼ņØś ĒÖĢļīĆļĪ£ ņĀ£ĻĘĀ ņ╣śļŻīļŖö ņĢ×ņ£╝ļĪ£ ĒÅŁļ░£ņĀüņ£╝ļĪ£ ļŖśņ¢┤ļéĀ Ļ░ĆļŖźņä▒ņØ┤ ļåÆļŗż. Ēśäņ×¼ ņØ╝ņ░© ņ╣śļŻīļĪ£ļŖö 1998ļģä ļīĆĒĢ£ņāüļČĆņ£äņןĻ┤Ć┬ĘĒŚ¼ļ”¼ņĮöļ░ĢĒä░ĒĢÖĒÜīņŚÉņä£ ņĀ£ņŗ£ĒĢ£ amoxicillin 2.0 g, proton pump inhibitor (PPI) ĻĘĖļ”¼Ļ│Ā clarithromycin 1.0 gņØ┤ļéś metronidazole 1.0 gņØä ņØ┤ņÜ®ĒĢ£ ņé╝ņĀ£ņÜöļ▓ĢņØä ņé¼ņÜ®ĒĢśĻ│Ā ņ׳ļŗż. ĒĢśņ¦Ćļ¦ī ņĄ£ĻĘ╝ ĒĢŁņāØņĀ£ ļé┤ņä▒ņŚÉ ņØśĒĢ£ ņĀ£ĻĘĀņ£© Ļ░Éņåī ņČöņäĖņŚÉ ļīĆĒĢ£ ņŚ░ĻĄ¼ļōżļÅä ļ¦ÄņØ┤ ļ│┤Ļ│ĀļÉśņŚłĻ│Ā, ļŹöņÜ▒ņØ┤ ņØ╝ņ░© ņĀ£ĻĘĀ ņ╣śļŻī ņŗżĒī© Ēøä ņØ┤ņ░© ņĀ£ĻĘĀ ņ╣śļŻīļĪ£ ņé¼ņÜ®ļÉśļŖö PPI, bismuth, tetracycline, metronidazoleņØś ņé¼ņĀ£ņÜöļ▓ĢņŚÉ ļīĆĒĢ£ ņĀ£ĻĘĀņ£©ļ¦łņĀĆļÅä 2000ļģä ņ┤łļ░śņŚÉ 90% ņØ┤ņāüņØ┤ņŚłļŹś Ļ▓āņØ┤ 2000ļģäļīĆ ņżæļ░ś ņØ┤Ēøä ņĀÉņĀÉ ņĀĆĒĢśļÉśĻ│Ā ņ׳ļŖö ņŗżņĀĢņØ┤ļŗż[3-5]. ņØ┤ļ¤¼ĒĢ£ ņĀäļ░śņĀüņØĖ ņĀ£ĻĘĀņ£© Ļ░ÉņåīņØś ņøÉņØĖņ£╝ļĪ£ļŖö ĒĢŁņāØņĀ£ ļé┤ņä▒, ĒÖśņ×ÉņØś ļéśņØ┤, ĒØĪņŚ░ ņŚ¼ļČĆ, ņłÖņŻ╝ ļ®┤ņŚŁņØś ņ░©ņØ┤, ĻĖ░ņĀĆņ¦łĒÖś, ņł£ņØæļÅä Ļ░Éņåī ļō▒ņØ┤ ņ׳ņ¦Ćļ¦ī ņØ┤ ņżæ ĒĢŁņāØņĀ£ ļé┤ņä▒ņØ┤ Ļ░Ćņן ņżæņÜöĒĢ£ ņØĖņ×ÉļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[5-7].
1997ļģä ņĢäņŗ£ņĢä-Ēā£ĒÅēņ¢æ ĒĢ®ņØś ļ│┤Ļ│Āņä£ņŚÉņä£ ņØ┤ņāüņĀüņØĖ ņĀ£ĻĘĀ ņ╣śļŻīļŖö ņĀ£ĻĘĀņ£©ņØ┤ intention-to-treat ļČäņäØņ£╝ļĪ£ 80% ņØ┤ņāü, per-protocol ļČäņäØņ£╝ļĪ£ 90% ņØ┤ņāü ļÉśņ¢┤ņĢ╝ ĒĢ£ļŗżĻ│Ā ĒĢśņśĆņ£╝ļéś[8], ņŗżņĀ£ ĻĄŁļé┤ņŚÉņä£ ĻĘ╝ļל ļ│┤Ļ│ĀļÉśļŖö ņĀ£ĻĘĀ ņ╣śļŻīņØś ņĀ£ĻĘĀņ£©ņØĆ ņØ┤ņŚÉ ļ»Ėņ╣śņ¦Ć ļ¬╗ĒĢśĻ│Ā ņ׳ļŗż. ņāłļĪ£ņÜ┤ ĒĢŁņāØņĀ£ņØś ņĪ░ĒĢ®ņ£╝ļĪ£ ņØ┤ņĀäļ│┤ļŗżļŖö ņóŗņØĆ ņĀ£ĻĘĀņ£©ņØä ļ│┤ņØ╝ ņłśļŖö ņ׳ņ¦Ćļ¦ī Ļ▓ĮņÜ░ņŚÉ ļö░ļØ╝ņä£ļŖö ņāłļĪ£ņÜ┤ ĒĢŁņāØņĀ£ņØś ļé┤ņä▒ņØä ņØ╝ņ£╝ĒéżļŖö Ļ│äĻĖ░Ļ░Ć ļÉ£ļŗżļŖö Ļ▓āņØä ņśłņāüĒĢśĻ│Ā ņ׳ļŗż. ņŗżņĀ£ļĪ£ ļīĆļ¦īņØś Ļ▓ĮņÜ░ņŚÉņä£ ĻĘĖ ņśłļź╝ ļ│╝ ņłś ņ׳ļŖöļŹ░[9], ņĀ£ĒĢ£ņĀüņØ┤ļ®┤ņä£ ņĀüņĀłĒĢ£ ĒĢŁņāØņĀ£ ņé¼ņÜ®ņØ┤ Ēśäņ×¼ļĪ£ļŖö Ļ░Ćņן ņØ┤ņāüņĀüņØ┤ļØ╝ ņāØĻ░üĒĢśļ®░ ņØ┤ņŚÉ ņØ╝ņ░© ņĀ£ĻĘĀ ņÜöļ▓ĢņØä ņŗżņŗ£ĒĢśĻĖ░ ņĀäņŚÉ ņĀ£ņØ╝ ļ¼ĖņĀ£Ļ░Ć ļÉśļŖö clarithromycinņØś ļé┤ņä▒ Ļ▓Ćņé¼ļź╝ ņŗżņŗ£ĒĢśĻ│Ā ņØ┤ņŚÉ ļö░ļØ╝ ņĀüņĀłĒĢ£ ņ╣śļŻī ņĢĮņĀ£ļź╝ ņäĀĒāØĒĢśļ®┤ ņĀ£ĻĘĀņ£©ņØä 90% ņØ┤ņāüņ£╝ļĪ£ ļåÆņØ╝ ņłś ņ׳ņØä Ļ▓āņ£╝ļĪ£ ĻĖ░ļīĆĒĢśĻ│Ā ņ׳ļŗż. ņĄ£ĻĘ╝ Ļ░£ņĀĢļÉ£ Ļ│Āņŗ£ņŚÉ ļö░ļØ╝ H. pylori ņĀ£ĻĘĀ ņĀäņŚÉ ļ»Ėļ”¼ clarithromycin ļé┤ņä▒ņØä ĒīÉļŗ©ĒĢĀ ņłś ņ׳Ļ▓ī ļÉśņŚłĻ│Ā, ņĀüņĀłĒĢ£ ĒĢŁņāØņĀ£ļź╝ ņé¼ņÜ®ĒĢ©ņ£╝ļĪ£ņŹ© ĒĢŁņāØņĀ£ ļé©ņÜ®ņØä ņżäņØ╝ ņłś ņ׳ņ£╝ļ®┤ņä£ ņØ┤ņāüņĀüņØĖ ņĀ£ĻĘĀņ£©ņŚÉ ņĀæĻĘ╝ĒĢĀ ņłś ņ׳ļŖö Ļ░ĆļŖźņä▒ņØä ņŚ┤Ļ▓ī ļÉśņŚłļŗż.
ļ│Ė ļĪĀ
1. H. pyloriņØś ĒĢŁņāØņĀ£ ļé┤ņä▒ņØś ļ│ĆĒÖö
ClarithromycinņØĆ macrolide Ļ│äņŚ┤ņØś ĒĢŁņāØņĀ£ļĪ£ erythromycinņØś 6ļ▓ł hydroxylĻĖ░ļź╝ methylation ņŗ£Ēé© ļ░śĒĢ®ņä▒ ĒĢŁņāØņĀ£ņØ┤ļŗż. ņäĖĻĘĀņØś ļ”¼ļ│┤ņå£(ribosome)ņŚÉ Ļ▓░ĒĢ®ĒĢśņŚ¼ ļŗ©ļ░▒ņ¦ł ņāØņä▒ņØä ņ¢ĄņĀ£ĒĢśĻ▓ī ļÉśļŖöļŹ░, ņØ┤ Ļ│äņŚ┤ņØś ļŗżļźĖ ĒĢŁņāØņĀ£ņŚÉ ļ╣äĒĢśņŚ¼ ņé░ņä▒ ĒÖśĻ▓ĮņŚÉņä£ļÅä ņĢłņĀĢņä▒ņØ┤ ļåÆĻ│Ā ĒØĪņłśņ£©ņØ┤ ļåÆņØĆ ņןņĀÉņØ┤ ņ׳ļŗż. ĒĢ£ĒÄĖ, ņĀ£ĻĘĀņŚÉ ņé¼ņÜ®ĒĢśĻ│Ā ņ׳ļŖö ĒĢŁņāØņĀ£ļōżņØś Ļ░üĻ░üņØś ļé┤ņä▒ļźĀņØä ļ│┤ļ®┤ 2000ļģä ņØ┤ņĀäņŚÉļŖö metronidazole, clarithromycin, amoxicillinņŚÉ ļīĆĒĢ£ ļé┤ņä▒ļźĀņØ┤ Ļ░üĻ░ü 40.6%, 5.9%, 0%ņśĆņ£╝ļéś[10,11], 2003ļģäņŚÉļŖö 66.2%, 13.8%, 18.5%ļĪ£ ņ”ØĻ░ĆĒĢśņśĆĻ│Ā[12], 2007~2009ļģäņŚÉļŖö 27.6%, 38.5%, 4.8%ļĪ£ metronidazole, amoxicillinņŚÉ ļīĆĒĢ£ ļé┤ņä▒ņØĆ Ļ░ÉņåīĒĢśņśĆņ£╝ļéś clarithromycinņŚÉ ļīĆĒĢ£ ļé┤ņä▒ļźĀņØĆ ĻŠĖņżĆĒ׳ ņ”ØĻ░ĆĒĢśļŖö ņČöņäĖņŚÉ ņ׳ļŗż[13]. ņĄ£ĻĘ╝ 10ļģä ņØ┤ļé┤ņŚÉ ņłśĒ¢ēļÉ£ ņŚ░ĻĄ¼ņØś clarithromycinņŚÉ ļīĆĒĢ£ ļé┤ņä▒ļźĀ(2007Ōł╝2009ļģä)ņØ┤ 38.5%ļĪ£ ĻĖēĻ▓®Ē׳ ņ”ØĻ░ĆĒĢśņśĆļŗżļŖö ņĀÉņØĆ ļåĆļØ╝ņÜ┤ ņØ╝ņØ┤ļŗż. ļŗżļ¦ī ņŚ░ĻĄ¼ņ×ÉņŚÉ ļö░ļØ╝ ļŗżņåī ņ░©ņØ┤ļŖö ņ׳ņ£╝ļéś clarithromycin ļé┤ņä▒ņØĆ ļīĆņ▓┤ņĀüņ£╝ļĪ£ ņ”ØĻ░ĆĒĢśĻ│Ā ņ׳ņ£╝ļ®░, 2011ļģä ņŗ£Ē¢ēļÉ£ ļŗżĻĖ░Ļ┤Ć ņŚ░ĻĄ¼ņŚÉņä£ļÅä clarithromycin ļé┤ņä▒ļźĀņØä 26.3%ļĪ£ ļ│┤Ļ│ĀĒĢśņśĆļŖöļŹ░[14], ņØ┤ļ¤¼ĒĢ£ ņĀÉņØä Ļ░ÉņĢłĒĢśļ®┤ ņĄ£ĻĘ╝ Ēæ£ņżĆ ņé╝ņĀ£ņÜöļ▓Ģ ņ╣śļŻī ņŗżĒī©ņØś ņŻ╝ņÜöĒĢ£ ņøÉņØĖņØ┤ clarithromycinņŚÉ ļīĆĒĢ£ ļé┤ņä▒ņ×äņØä ņĢī ņłś ņ׳ļŗż. ņŻ╝ļ¬®ĒĢĀ Ļ▓āņØĆ amoxicillinĻ│╝ clarithromycinņŚÉ ļ¬©ļæÉ ļé┤ņä▒ņØ┤ ņŚåļŖö Ļ▓ĮņÜ░ņŚÉļŖö Ēæ£ņżĆ ņé╝ņĀ£ņÜöļ▓ĢņØś ņĀ£ĻĘĀņ£©ņØĆ 95% ļé┤ņÖĖņØĖ ļ░śļ®┤, clarithromycinņŚÉ ļé┤ņä▒ņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ņŚÉņä£ ņĀ£ĻĘĀņ£©ņØĆ 43Ōł╝65% ņĀĢļÅäļĪ£ ļ│┤Ļ│ĀĒĢśĻ│Ā ņ׳ņ¢┤ clarithromycinņØś ļé┤ņä▒ņØ┤ ņĀ£ĻĘĀ ņ╣śļŻī ņŗżĒī©ņŚÉ Ļ░Ćņן Ēü░ ņśüĒ¢źņ×äņØä ņ”Øļ¬ģĒĢśņśĆļŗż[13,15].
ļæÉ Ļ░Ćņ¦Ć ņØ┤ņāüņØś ĒĢŁņāØņĀ£ņŚÉ ļé┤ņä▒ņØä ļ│┤ņØ┤ļŖö ļŗżņĢĮņĀ£ ļé┤ņä▒ H. pylori ĻĘĀņŻ╝ļÅä ņ¦ĆņåŹņĀüņ£╝ļĪ£ ĻŠĖņżĆĒ׳ ņ”ØĻ░ĆĒĢśĻ│Ā ņ׳ļŗż. ļŗżņĢĮņĀ£ ļé┤ņä▒ĻĘĀņØĆ 1987ļģä 24%, 1994ļģä 33%, 2003ļģä 47.7%ļĪ£ ņ”ØĻ░ĆĒĢśņśĆņ£╝ļ®░[16], ņØ┤Ēøä ņŚ░ĻĄ¼ņŚÉņä£ļÅä 2007Ōł╝2009ļģä 40.3%ļĪ£ ņ”ØĻ░ĆĒĢśņśĆļŗż[13]. ņĄ£ĻĘ╝ņØś ņŚ░ĻĄ¼ņŚÉņä£ļÅä 2011Ōł╝2012ļģä 23.4%ļĪ£ ļéśĒāĆļé¼ļŗż[17]. ļŗżņĢĮņĀ£ ļé┤ņä▒ņØä ļ│┤ņØ┤ļŖö ĒĢŁņāØņĀ£ņØś ņĪ░ĒĢ®ņØĆ ļ¦żņÜ░ ļŗżņ¢æĒĢ£ļŹ░, ĒŖ╣Ē׳ ņĀ£ĻĘĀ ņ╣śļŻīņØś ņØ╝ņ░© ņĢĮņĀ£ļĪ£ ņé¼ņÜ®ļÉśĻ│Ā ņ׳ļŖö amoxicillinĻ│╝ clarithromycinņŚÉ ļÅÖņŗ£ ļé┤ņä▒ņØä ļéśĒāĆļéĖ ĻĘĀņŻ╝ļŖö 2011ļģä ņŚ░ĻĄ¼ņŚÉņä£ 4.0%ņśĆļŗż[14]. ClarithromycinĻ│╝ metronidazoleņŚÉ ĒĢ©Ļ╗ś ļé┤ņä▒ņØä ļ│┤ņØ┤ļŖö ĻĘĀņŻ╝ ļśÉĒĢ£ 2013ļģä ņŚ░ĻĄ¼ņŚÉņä£ 6.1%ļĪ£ ļéśĒāĆļé¼ļŗż[17].
2. H. pylori ņØś clarithromycin ļé┤ņä▒ ĻĖ░ņĀä
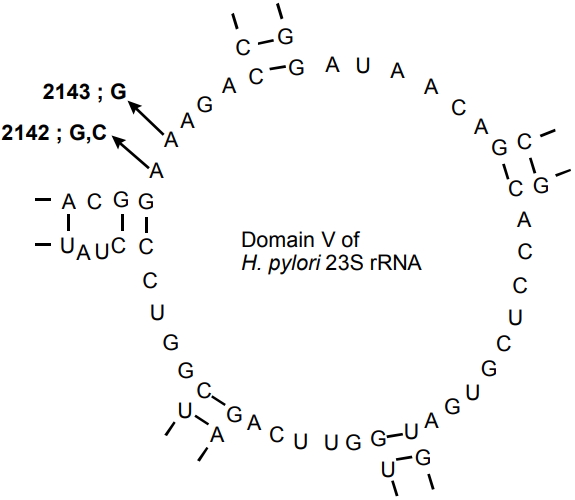
ClarithromycinņØĆ H. pyloriņŚÉ ļīĆĒĢśņŚ¼ ņé¼ņÜ® Ļ░ĆļŖźĒĢ£ Ļ░Ćņן Ļ░ĢļĀźĒĢ£ ĒĢŁņāØņĀ£ļĪ£ ļé©ņĢä ņ׳ņ£╝ļ®░ ņĀĢĻĘĀ ĒÖ£ņä▒ņØĆ 23S ribosomal RNA (rRNA) geneņŚÉ Ļ▓░ĒĢ®, ņ×æņÜ®ņØä ĒĢśņŚ¼ ļŗ©ļ░▒ņ¦ł ĒĢ®ņä▒ņØä ļ░®ĒĢ┤ĒĢśļŖö ĻĖ░ņĀäņØä Ļ░Ćņ¦ĆĻ│Ā ņ׳ļŖö ņĢĮņĀ£ņØ┤ļŗż. ņżæĒĢ®ĒÜ©ņåīņŚ░ņćäļ░śņØæĻ▓Ćņé¼(polymerase chain reaction, PCR) ĻĖ░ļ░ś Ļ┤æļ▓öņ£ä ņŚ░ĻĄ¼ņŚÉ ļö░ļź┤ļ®┤, 23S rRNAņØś V ņśüņŚŁņŚÉ ņĮöļō£ ņśüņŚŁņØś ņĀÉ ļÅīņŚ░ļ│ĆņØ┤(point mutation)Ļ░Ć ņäĖĻĘĀ ļé┤ņä▒ņØä ņØ╝ņ£╝ĒéżļŖö Ļ▓āņ£╝ļĪ£ ļ░ØĒśĆņĪīļŗż(Fig. 1) [18]. ņØ┤ļ¤¼ĒĢ£ ļÅīņŚ░ļ│ĆņØ┤ļŖö clarithromycinĻ│╝ ĒŖ╣ņĀĢ ĒĢŁņāØņĀ£ Ļ┤ĆļĀ© ļŗ©ļ░▒ņ¦ł ĒĢ®ņä▒ņŚÉ ņé¼ņÜ®ļÉśļŖö ribosomal subunit ņé¼ņØ┤ņØś Ļ▓░ĒĢ®ņØä ņ¢ĄņĀ£ĒĢĀ ņłś ņ׳ļŗż. ļśÉĒĢ£ H. pyloriļŖö ņ£ĀņČ£ ņ▒äļäÉ(efflux channel)ņØä ĒåĄĒĢśņŚ¼ ĒĢŁņāØņĀ£ļź╝ ņäĖĻĘĀ ļ░¢ņ£╝ļĪ£ ļ╣Āļź┤Ļ▓ī ņØ┤ļÅÖņŗ£ņ╝£ ĒĢŁņāØņĀ£Ļ░Ć ļ”¼ļ│┤ņå£ņŚÉ Ļ▓░ĒĢ®ĒĢśļŖö Ļ▓āņØä ļ░®ĒĢ┤ĒĢ£ļŗż[19]. ļö░ļØ╝ņä£ Ēæ£ņżĆ ņé╝ņĀ£ņÜöļ▓ĢņØ┤ļéś ņł£ņ░© ņ╣śļŻī(sequential therapy)ņŚÉņä£ ņ▓śņØī ņé¼ņÜ®ļÉśļŖö amoxicillinņØĆ ņ£ĀņČ£ ņ▒äļäÉņØä ņĢĮĒÖöņŗ£ņ╝£ ņØ┤ĒøäņŚÉ Ēł¼ņŚ¼ļÉśļŖö clarithromycinņØś ĒÜ©Ļ│╝ļź╝ Ē¢źņāüņŗ£ĒéżĻ│Ā ļé┤ņä▒ņØä ņ¢ĄņĀ£ĒĢśĻ▓ī ļÉ£ļŗż[20,21].
3. H. pyloriņØś clarithromycin ĒĢŁņāØņĀ£ Ļ░Éņłśņä▒ Ļ▓Ćņé¼
PCR ĻĖ░ļ░ś Ļ▓Ćņé¼Ļ░Ć ļ│┤ĒÄĖĒÖöļÉśĻĖ░ ņĀäņŚÉļŖö ņŻ╝ļĪ£ clarithromycinņŚÉ ļīĆĒĢ£ ļé┤ņä▒ņØä ņ¦äļŗ©ĒĢśĻĖ░ ņ£äĒĢśņŚ¼ ļ░░ņ¢æ ļ░Å ļööņŖżĒü¼ ĒÖĢņé░ļ▓Ģ(disk diffusion method), E-test ļō▒ņØś ļ░®ļ▓ĢņØ┤ ņØ┤ņÜ®ļÉśņ¢┤ ņÖöļŗż. ņĄ£ņåī ņ¢ĄņĀ£ ļåŹļÅä(minimal inhibitory concentration)ļŖö ĒĢŁĻĘĀļĀźņØä ņĖĪņĀĢĒĢśļŖö ņ¦ĆĒæ£ļĪ£ņä£ ĒĢŁņāØņĀ£ Ļ░Éņłśņä▒ Ļ▓Ćņé¼ņŚÉņä£ ļ»ĖņāØļ¼╝ņØś ļ▓łņŗØņØä ņ¢ĄņĀ£ĒĢĀ ņłś ņ׳ļŖö ĒĢŁņāØņĀ£ņØś ņĄ£ņĀĆ ļåŹļÅäļĪ£ ņĀĢņØśĒĢ£ļŗż[16]. ĻĘĖļ¤¼ļéś H. pyloriņØś ĒĢŁņāØņĀ£ņŚÉ ļīĆĒĢ£ ņĄ£ņåī ņ¢ĄņĀ£ ļåŹļÅäļŖö ļ│┤Ļ│Āņ×ÉņŚÉ ļö░ļØ╝ ļ¦ÄņØĆ ņ░©ņØ┤ļź╝ ļ│┤ņØ┤ļŖöļŹ░, ņ¦ĆņŚŁļ¦łļŗż ĻĘĀņŻ╝ņØś ņ░©ņØ┤Ļ░Ć ņĪ┤ņ×¼ĒĢśĻ│Ā ĻĘĀņŻ╝ņØś ļ░░ņ¢æĒĢśļŖö ņĪ░Ļ▒┤ņØ┤ Ļ╣īļŗżļĪ£ņÜĖ ļ┐É ņĢäļŗłļØ╝ Ļ▓Ćņé¼ļ▓ĢņØ┤ ĒåĄņØ╝ļÉśņ¦Ć ņĢŖļŖö ņĀÉņŚÉņä£ ĻĖ░ņØĖĒĢ£ļŗż[22,23]. ņĀĢĒÖĢĒĢ£ ĻĘĀņŻ╝ņØś ļ░░ņ¢æņØä ņ£äĒĢśņŚ¼ Ļ▓Ćņé¼ ņĀä ņĀüņ¢┤ļÅä 2ņŻ╝Ļ░äņØś PPI ļ│ĄņÜ® ļ░Å 4ņŻ╝Ļ░äņØś ĒĢŁņāØņĀ£ ļ│ĄņÜ®ņØ┤ ņĀ£ĒĢ£ļÉśļ®░, ņ▒äņĘ©ĒĢ£ ņĪ░ņ¦üņØĆ Ļ░ĆļŖźĒĢ£ ļ╣Āļź┤Ļ▓ī ņ▓śļ”¼ļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż. ļśÉĒĢ£ ļ░░ņ¢æĻ▓Ćņé¼ļŖö ļ»╝Ļ░ÉļÅäļŖö 73% ņØ┤ĒĢśļĪ£ ļé«ļŗżļŖö ļŗ©ņĀÉņØ┤ ņ׳ļŖö ļ░śļ®┤ clarithromycin ļé┤ņä▒ ņĀäļ░śņØä ĒÅēĻ░ĆĒĢĀ ņłś ņ׳ļŗżļŖö ņןņĀÉņØ┤ ņ׳ļŗż[24,25].
PCR ļ░®ļ▓ĢņØ┤ H. pylori Ļ░ÉņŚ╝ņØä ĒīÉļŗ©ĒĢśļŖö Ļ▓Ćņé¼ļĪ£ņä£ ņÜöņ¢æĻĖēņŚ¼Ļ░Ć ĒÖĢļīĆļÉśļ®┤ņä£ ļ│┤ĒÄĖĒÖöļÉśņŚłļŖöļŹ░, ņØ┤ļĪ£ņŹ© Ļ▓Ćņé¼ņØś ļ»╝Ļ░ÉļÅä ļ░Å ņ¦äļŗ©ņØś ņĀĢĒÖĢļÅäļŖö ļłłļČĆņŗ£Ļ▓ī ņāüņŖ╣ĒĢśņśĆļŗż. ļŹöņÜ▒ņØ┤ clarithromycinņŚÉ ļīĆĒĢ£ ļé┤ņä▒ņØĆ ļīĆļČĆļČä 23S rRNA geneņØś 2142 Ēś╣ņØĆ 2143 ņ£äņ╣śņØś ņĀÉ ļÅīņŚ░ļ│ĆņØ┤ņŚÉ ņØśĒĢśņŚ¼ ņØ╝ņ¢┤ļéśļŖöļŹ░, PCR ļ░®ļ▓ĢņØä ņØ┤ņÜ®ĒĢ£ Ļ▓Ćņé¼ļĪ£ ĒĢŁņāØņĀ£ ļé┤ņä▒ļÅä ņśłņĖĪĒĢĀ ņłś ņ׳Ļ▓ī ļÉśņŚłļŗż. ņŻ╝ļĪ£ ņĀÉ ļÅīņŚ░ļ│ĆņØ┤ņØś ņ£äņ╣śļŖö ņŻ╝ļĪ£ ņŚ╝ĻĖ░ņä£ņŚ┤ 2142ņÖĆ 2143 ņ£äņ╣śņŚÉ adenineņØ┤ guanineņ£╝ļĪ£ ņ╣śĒÖśļÉśļŖö Ļ▓ĮņÜ░(A2142G, A2143G)ņØ┤ļ®░, ļō£ļ¼╝Ļ▓ī 2142 ņ£äņ╣śņŚÉ adenineņØ┤ cytosineņ£╝ļĪ£ ņ╣śĒÖśļÉśļŖö Ļ▓ĮņÜ░(A2142C)ņÖĆ ĻĘĖ ņÖĖņŚÉļÅä A2115G, G2141A, A2142T, T2182Cļź╝ ļ│┤Ļ│ĀĒĢśĻ│Ā ņ׳ļŗż[26,27]. ņ¦ĆņŚŁļ¦łļŗż ļÅīņŚ░ļ│ĆņØ┤ņØś ļČäĒżļŖö ļŗżņåī ņ░©ņØ┤Ļ░Ć ņ׳ļŖöļŹ░, ļ»ĖĻĄŁņŚÉņä£ A2142G, A2143G ļ│ĆņØ┤ļŖö Ļ░üĻ░ü 48~53%ņÖĆ 39~45%ņØ┤ļ®┤ņä£ A2142C ļ│ĆņØ┤ļŖö 0~7%ņØ┤Ļ│Ā, ņ£Āļ¤ĮņØĆ A2142G, A2143G ļ│ĆņØ┤Ļ░Ć Ļ░üĻ░ü 23~33%ņÖĆ 44~67%ņØ┤ļ®┤ņä£ A2142C ļ│ĆņØ┤ļŖö 2~10%ļĪ£ ļ│┤Ļ│ĀĒĢśņŚ¼ ļ»ĖĻĄŁĻ│╝ ņ£Āļ¤ĮņØś clarithromycin ļé┤ņä▒ņØś ņŻ╝ņÜö ļ│ĆņóģņØś ļČäĒżļŖö ņ£Āņé¼ĒĢśļŗż[28-30]. ĒĢśņ¦Ćļ¦ī ņØ╝ļ│ĖņŚÉņä£ļŖö A2143GņØś Ļ▓ĮņÜ░Ļ░Ć 90% ņØ┤ņāüņØ┤ļ®┤ņä£ A2142CļŖö ļ░£Ļ▓¼ļÉśņ¦Ć ņĢŖņĢśĻ│Ā[31,32], ņżæĻĄŁņØś ņŚ░ĻĄ¼ņŚÉņä£ļÅä ļ╣äļĪØ ņĀüņØĆ ņłśņØś ņŚ░ĻĄ¼ņØ┤ņ¦Ćļ¦ī A2143G ļ│ĆņØ┤Ļ░Ć Ļ▒░ņØś 100%ļØ╝Ļ│Ā ļ│┤Ļ│ĀĒĢśņśĆļŗż[33]. ĒÖŹņĮ®ņŚÉņä£ļŖö A2144G ļ│ĆņØ┤ ļ╣łļÅäĻ░Ć ļåÆņØĆ Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳Ļ│Ā[34], ĒĢ£ĻĄŁņØĆ 2004ļģä clarithromycin ļé┤ņä▒ņØĖ 10ĻĘĀņŻ╝ ņżæ 7ĻĘĀņŻ╝ņŚÉņä£ A2143G ļ│ĆņØ┤ļź╝ ļ│┤Ļ│ĀĒĢśņśĆļŖöļŹ░[16], 2005ļģäņŚÉ ņŗżņŗ£ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ļŖö clarithromycin ļé┤ņä▒ņØ┤ 20.2%ņØ┤ļ®┤ņä£ ļīĆļČĆļČäņØ┤ A2142GļØ╝Ļ│Ā ĒĢśņŚ¼ ņØ┤ņĀä Ļ▓░Ļ│╝ņÖĆļŖö ļŗżņåī ļŗżļź┤Ļ▓ī ļ│┤Ļ│ĀĒĢśņśĆļŗż[35]. ĻĘĖļ¤¼ļéś ņØ┤Ēøä ņŚ¼ļ¤¼ ņŚ░ĻĄ¼ņŚÉņä£ ļīĆļČĆļČäņØś clarithromycin ļé┤ņä▒ņØĆ ļīĆļČĆļČäņØ┤ A2143G ļ│ĆņØ┤ļĪ£ ĒÖĢņØĖļÉśņŚłļŗż[36-38]. ņØ┤ļ¤¼ĒĢ£ PCR ļ░®ļ▓ĢņØĆ 82~90% ņØ┤ņāüņ£╝ļĪ£ ņāüļīĆņĀüņ£╝ļĪ£ ļåÆņØĆ ļ»╝Ļ░ÉļÅä ļ░Å 95% ņØ┤ņāüņØś ĒŖ╣ņØ┤ļÅäļź╝ ļéśĒāĆļé┤ļŖö ņÜ░ņłśņä▒ņØ┤ ņ׳ļŖö Ļ▓Ćņé¼ņØ┤Ļ│Ā[39-41], ļŹöĻĄ░ļŗżļéś ļ░░ņ¢æĻ▓Ćņé¼ņŚÉņä£ ņĀ£ĒĢ£ļÉśļŖö clarithromycinņÖĆ quinoloneņØś ļÅÖņŗ£ ļé┤ņä▒ņØä ĒÖĢņØĖĒĢĀ ņłś ņ׳ļŖö ņןņĀÉņØ┤ ņ׳ļŗż[42].
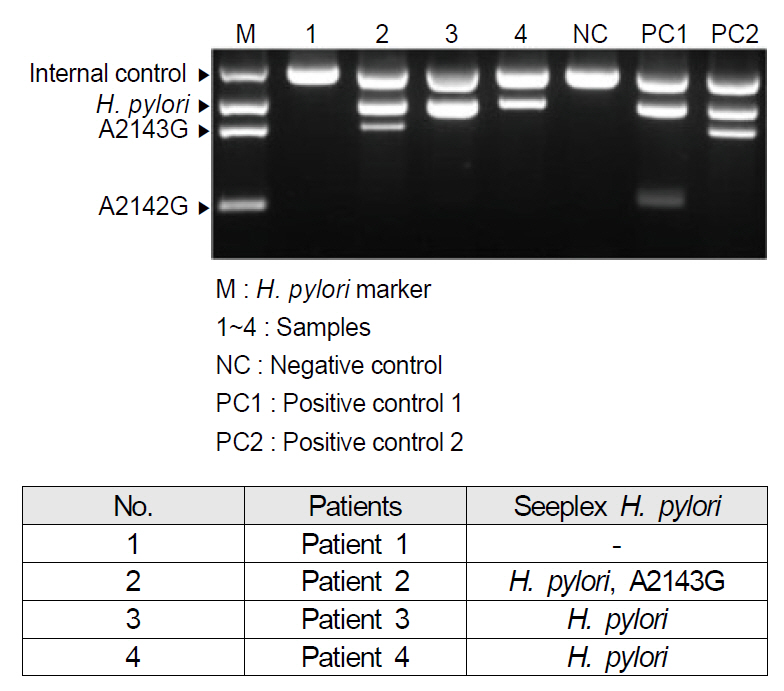
ĻĘĖļ¤¼ļéś ĻĖ░ļīĆņÖĆļŖö ļŗ¼ļ”¼ ņ£äņ¢æņä▒ ļ░Å ņ£äņØīņä▒ļźĀņØ┤ ļŗżņåī ĻĖ░ļīĆņŚÉ ļ»Ėņ╣śņ¦Ć ļ¬╗ĒĢśĻ│Ā ļśÉĒĢ£ ĒśäņŗżņĀüņ£╝ļĪ£ Ļ▓Ćņé¼ņØś ļ▓łĻ▒░ļĪ£ņøĆĻ│╝ Ļ│ĀĻ░ĆņØś ņןļ╣ä ĻĘĖļ”¼Ļ│Ā Ļ▓Ćņé¼ ņØĖļĀźņØä ņČöĻ░ĆļĪ£ ĒĢäņÜöĒĢśĻ▓ī ĒĢśņŚ¼ ļīĆĒśĢ ļ│æņøÉņØ┤ ņĢäļŗłļ®┤ Ļ░ÉĒ׳ Ļ▓Ćņé¼ļź╝ ĒĢśĻĖ░ ĒלļōĀ ņŗżņĀĢņØ┤ņŚłļŗż. ņØ┤ņÖĖņŚÉļÅä MutaREAL H. pylori kit, ClariRes realtime PCR assay, Seeplex ClaR-H. pylori ACE detection system ļō▒ņØ┤ clarithromycin ļé┤ņä▒ ņ¦äļŗ©ņØä ņ£äĒĢśņŚ¼ Ļ│ĀņĢłļÉśņŚłņ£╝ļ®░[43], ĒŖ╣Ē׳ ņĄ£ĻĘ╝ņŚÉ ņåīĻ░£ļÉ£ DPO-based multiplex PCR (Seegene Inc., Seoul, Korea)ņØĆ ĻĖ░ņĪ┤ņØś PCR Ļ▓Ćņé¼ņŚÉ ļ╣äĒĢśņŚ¼ polydeoxynosine linkerļĪ£ ņŚ░Ļ▓░ļÉ£ ĻĖĖņØ┤Ļ░Ć ļŗżļźĖ ļæÉ Ļ░£ņØś primerļź╝ ņé¼ņÜ®ĒĢśĻĖ░ ļĢīļ¼ĖņŚÉ ļ╣äĒŖ╣ņØ┤ņĀüņØĖ PCR ņé░ļ¼╝ņØä ņāØņä▒ĒĢśņ¦Ć ņĢŖņĢä ĻĖ░ņĪ┤ PCRļ│┤ļŗż ņ£äņ¢æņä▒ļźĀņØä ļé«ņČöņŚłļŗż[38,44]. ņŚ░ĻĄ¼ņŚÉ ļö░ļź┤ļ®┤ DPO-PCRņØś ļ»╝Ļ░ÉļÅäņÖĆ ĒŖ╣ņØ┤ļÅäļŖö Ļ░üĻ░ü 87.5%, 91.3%ņśĆĻ│Ā ņ¢æņä▒ ņśłņĖĪļźĀ ļ░Å ņØīņä▒ ņśłņĖĪļźĀ, ņĀĢĒÖĢļÅäļŖö Ļ░üĻ░ü 84.0%, 93.3%, 90.0%ņśĆļŗż[45]. ļśÉĒĢ£ ĻĘ£Ļ▓®ĒÖöļÉśņ¢┤ Ļ▓Ćņé¼ļź╝ Ļ░äļŗ©ĒĢśĻ▓ī ĒĢśņśĆĻ│Ā Ļ▓Ćņé¼ļ╣äņÜ®ņØś ņĀłĻ░ÉņØä Ļ░ĆņĀĖņśżĻ▓ī ĒĢśņśĆļŗż. DPO-PCRņŚÉņä£ļŖö ņ¦äļŗ©ļ┐Éļ¦ī ņĢäļŗłļØ╝ clarithromycin ļé┤ņä▒ļÅä ļŹöļČłņ¢┤ ĒīīņĢģĒĢĀ ņłś ņ׳Ļ▓ī ņäżĻ│äļÉśņ¢┤ ņ׳ļŖöļŹ░, clarithromycin ļé┤ņä▒ņØś 80% ņØ┤ņāüņØä ņ░©ņ¦ĆĒĢśņŚ¼ ņŻ╝ņÜö ņøÉņØĖņ£╝ļĪ£ ņĢīļĀżņ¦ä A2142GņÖĆ A2143G ļ│ĆņØ┤ļź╝ ņĖĪņĀĢĒĢĀ ņłś ņ׳Ļ▓ī Ļ│ĀņĢłļÉśņŚłļŗż[46,47]. PCR ņé░ļ¼╝Ļ│╝ ClaR-HP markerļź╝ Ļ░üĻ░ü ņĀäĻĖ░ ņśüļÅÖĒĢ£ Ēøä ņ×ÉņÖĖņäĀ Ēł¼Ļ│╝ ņĪ░ļ¬ģĻĖ░ņŚÉņä£ ņ”ØĒÅŁļÉ£ ņ£ĀņĀäņ×Éļź╝ ĒÖĢņØĖĒĢ©ņ£╝ļĪ£ņŹ© ļé┤ņä▒ņØä ņśłņāüĒĢśĻ▓ī ļÉśļŖöļŹ░, ņ”ØĒÅŁļÉ£ DNA ņé░ļ¼╝ņŚÉņä£ 621 bp ņé░ļ¼╝ļ¦ī Ļ┤Ćņ░░ļÉśļ®┤ H. pylori wild-typeņ£╝ļĪ£ Ļ░ÉņŚ╝ņØä ņ¦äļŗ©ĒĢśĻ│Ā, 475 bpĻ░Ć ĒĢ©Ļ╗ś Ļ┤Ćņ░░ļÉśļ®┤ A2143G ļ│ĆņØ┤ĒśĢ, 194 bpĻ░Ć ĒĢ©Ļ╗ś Ļ┤Ćņ░░ļÉśļ®┤ A2142G ļ│ĆņØ┤ĒśĢņ£╝ļĪ£ ĒĢ┤ņäØĒĢĀ ņłś ņ׳ļŗż(Fig. 2).
ļśÉĒĢ£ ļö░ļĪ£ Ļ▓Ćņ▓┤ļź╝ ņĪ░ņ¦üĻ▓Ćņé¼ļź╝ ĒåĄĒĢśņŚ¼ ņĀ£Ļ│ĄĒĢĀ ĒĢäņÜöĻ░Ć ņŚåĻ│Ā, ņŗĀņåŹ ņÜöņåīļČäĒĢ┤ĒÜ©ņåī Ļ▓Ćņé¼(rapid urease test) kitņŚÉ ļŗ┤Ļ▓© ņ׳ļŖö ņĪ░ņ¦üņØä ĻĘĖļīĆļĪ£ Ļ▓Ćņé¼ņŗżņŚÉ ļ│┤ļāäņ£╝ļĪ£ņŹ© ļ▓łĻ▒░ļĪ£ņøĆņØä ļŹ£Ļ▓ī ņäżĻ│äļÉśņŚłļŗż[38,48]. DPO-PCRņØĆ ņŗĀņåŹ ņÜöņåīļČäĒĢ┤ĒÜ©ņåī Ļ▓Ćņé¼ ņØīņä▒ņØś ņĪ░ņ¦üņŚÉņä£ļÅä Ļ▓ĆņČ£ļÉśĻĖ░ļÅä ĒĢśņŚ¼ ņ£äņØīņä▒ņØä ņżäņØ┤Ļ│Ā ņ×¼ņĪ░ņ¦üĻ▓Ćņé¼ņØś ĒĢäņÜöņä▒ņØä Ļ░Éņåīņŗ£ņ╝░ļŗż. Ļ▓░Ļ│╝ņĀüņ£╝ļĪ£ DPO-PCR testļŖö ņ¦äļŗ©ļ┐É ņĢäļŗłļØ╝ H. pylori 23S rRNA geneņŚÉņä£ņØś ļ│ĆņØ┤ļź╝ ļ╣Āļź┤Ļ▓ī sequencingĒĢ©ņ£╝ļĪ£ņŹ© ĒÖśņ×ÉņØś ņØ╝ņ░© ņ╣śļŻī ņĢĮņĀ£ļź╝ ņäĀĒāØĒĢśļŖöļŹ░ ļÅäņøĆņØä ņŻ╝Ļ▓ī ļÉ£ļŗż.
4. H. pyloriņØś clarithromycin ĒĢŁņāØņĀ£ Ļ░Éņłśņä▒ Ļ▓Ćņé¼ņŚÉ ļö░ļźĖ ņ╣śļŻī
ClarithromycinņŚÉ ļīĆĒĢ£ ļåÆņØĆ ņłśņżĆņØś ļé┤ņä▒ņØĖ Ļ▓ĮņÜ░ļŖö H. pylori Ļ░ÉņŚ╝ņØä ņ╣śļŻīĒĢśĻ│Ā ņ¢ĄņĀ£ĒĢśļŖö ļäōņØĆ ņØśļ»ĖņØś ņāłļĪ£ņÜ┤ ņ╣śļŻīļ▓ĢņØä ņ░ŠņĢäļé┤ļŖö Ļ▓āņØ┤ ņżæņÜöĒĢśļŗż. Maastricht V/Florence ņ¦äļŻīņ¦Ćņ╣©ņŚÉņä£ļŖö clarithromycin ļé┤ņä▒ļźĀņØ┤ 15% ņØ┤ņāüņ£╝ļĪ£ ļåÆņØĆ ņ¦ĆņŚŁņŚÉņä£ļŖö bismuth ņé¼ņĀ£ņÜöļ▓ĢņØ┤ļéś ļÅÖņŗ£ ņ╣śļŻīļ▓ĢņØä ņäĀĒāØĒĢĀ Ļ▓āņØä ņČöņ▓£ĒĢśĻ│Ā ņ׳ļŖöļŹ░[49], ņĄ£ĻĘ╝ ņÜ░ļ”¼ļéśļØ╝ņØś clarithromycin ļé┤ņä▒ņØ┤ ņĢĮ 30%ļØ╝ļŖö ļ│┤Ļ│Āļź╝ ņ░ĖĻ│ĀĒĢ£ļŗżļ®┤[50] clarithromycinņØä ĻĖ░ļ│Ėņ£╝ļĪ£ ĒĢ£ ĻĖ░ņĪ┤ņØś ņé╝ņĀ£ņÜöļ▓ĢņØä ņØ╝ņ░© ņ╣śļŻīļĪ£ ņ£Āņ¦ĆĒĢśĻĖ░ļ│┤ļŗżļŖö ĒĢŁņāØņĀ£ Ļ░Éņłśņä▒ Ļ▓Ćņé¼ Ļ▓░Ļ│╝ļź╝ ĒåĀļīĆļĪ£ ĒĢ£ ņ╣śļŻī Ļ│äĒÜŹ ņłśļ”ĮņØ┤ ĒĢäņÜöĒĢśļŗż.
ņĄ£ĻĘ╝ ĻĄŁļé┤ņØś ļ│┤Ļ│ĀņŚÉ ļö░ļź┤ļ®┤ ņĀ£ĻĘĀ ņĀä DPO-PCR Ļ▓Ćņé¼ļź╝ ĒåĄĒĢśņŚ¼ clarithromycin ļé┤ņä▒ņŚÉ ļīĆĒĢ£ ņĀÉ ļÅīņŚ░ļ│ĆņØ┤ļź╝ ļ»Ėļ”¼ ņĢīĻ│Ā ļ¦×ņČżņĀ£ĻĘĀņØä ĒĢśņśĆņØä ļĢī, per-protocol ļČäņäØ Ļ▓░Ļ│╝ 91.0%ņØś ņĀ£ĻĘĀ ņä▒Ļ│ĄļźĀņØä ļ│┤ņŚ¼ņŻ╝ņŚłļŗż[51]. ĒĢśņ¦Ćļ¦ī Ēśäņ×¼Ļ╣īņ¦Ć ĻĄŁļé┤ņŚÉņä£ clarithromycin ļé┤ņä▒ņØ┤ ĒÖĢņØĖļÉ£ ĒÖśņ×ÉņŚÉņä£ ņØ╝ņ░© ņ╣śļŻī ņĢĮņĀ£ņŚÉ ļīĆĒĢ£ Ēæ£ņżĆ Ļ░ĆņØ┤ļō£ļØ╝ņØĖņØĆ ņĀĢļ”ĮļÉśņ¦Ć ņĢŖņĢśļŗż. ņØ╝ļ░śņĀüņ£╝ļĪ£ļŖö ņĀ£ĻĘĀ ņĀä clarithromycin ļé┤ņä▒ņØä ĒÖĢņØĖĒĢ£ Ļ▓ĮņÜ░ņŚÉ ņäĀĒāØĒĢĀ ņłś ņ׳ļŖö ņĢĮņĀ£ļŖö metronidazoleņØä ĻĘ╝Ļ░äņ£╝ļĪ£ ĒĢśļŖö ņé╝ņĀ£ņÜöļ▓ĢņØä ņäĀĒāØĒĢĀ ņłś ņ׳ņ£╝ļéś ļÅÖņŗ£ņŚÉ ņĪ┤ņ×¼ĒĢĀ ņłś ņ׳ļŖö ļŗżņĀ£ ļé┤ņä▒ ĻĘĀņŻ╝, ĒŖ╣Ē׳ metronidazoleņØś ļé┤ņä▒ņØä ļÅÖņŗ£ņŚÉ Ļ░Ćņ¦ĆĻ│Ā ņ׳ļŖö Ļ▓ĮņÜ░Ļ░Ć ļåÆņØĆ ņ¦ĆņŚŁņŚÉņä£ļŖö 14ņØ╝ ļÅÖņĢłņØś bismuthļź╝ ĻĘ╝Ļ░äņ£╝ļĪ£ ĒĢśļŖö Ļ│ĀņĀäņĀüņØĖ ņé¼ņĀ£ņÜöļ▓ĢņØä ņØ╝ņ░© ņĀ£ĻĘĀ ņÜöļ▓Ģņ£╝ļĪ£ ņäĀĒāØĒĢĀ ņłś ņ׳ļŗż. ĻĘĖļ¤¼ļéś ņØ┤ ņÜöļ▓ĢņØĆ ļ│ĄņÜ®ļ▓ĢņØ┤ ļ│Ąņ×ĪĒĢĀ ļ┐Éļ¦ī ņĢäļŗłļØ╝ ņĢĮņĀ£ ļČĆņ×æņÜ®ļÅä ļ¦ÄņĢäņä£ ĒÖśņ×ÉņØś ņł£ņØæļÅäĻ░Ć ļé«ļŗżļŖö ļŗ©ņĀÉņØ┤ ņ׳Ļ│Ā, ņØ╝ņ░© ņĀ£ĻĘĀ ņ╣śļŻīņŚÉ ņŗżĒī©ĒĢśņśĆņØä ļĢīņŚÉ ņØ┤ņ░© ņ╣śļŻī ņĢĮņĀ£ļź╝ ņäĀņĀĢĒĢśļŖö ļŹ░ ņ¢┤ļĀżņøĆņØ┤ ņ׳ļŗż. ĻĄŁļé┤ņØś ņŚ░ĻĄ¼ņŚÉņä£ clarithromycin ļé┤ņä▒ņØ┤ ĒÖĢņØĖļÉ£ ņØ╝ņ░© ņ╣śļŻīļĪ£ metronidazole ĒżĒĢ© ņé╝ņĀ£ņÜöļ▓ĢņØĆ ĻĖ░ņĪ┤ņØś bismuth ĒżĒĢ© ņé¼ņĀ£ņÜöļ▓ĢņŚÉ ļ╣äĒĢśņŚ¼ ņĀ£ĻĘĀņŚÉņä£ ĒåĄĻ│äņĀüņ£╝ļĪ£ ņ░©ņØ┤Ļ░Ć ņŚåĻ│Ā ļČĆņ×æņÜ® ņĖĪļ®┤ņŚÉņä£ļÅä ņÜ░ņøöĒĢ£ Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│ĀļÉśņŚłļŗż[52]. ĻĘĖļ¤¼ļéś ņØ┤ņŚÉ ļīĆĒĢ┤ņä£ļŖö Ē¢źĒøä ņČöĻ░ĆņĀüņØĖ ļīĆĻĘ£ļ¬© ņŚ░ĻĄ¼Ļ░Ć ĒĢäņÜöĒĢśļ®░ ĒĢÖĒÜī ņ░©ņøÉņŚÉņä£ ņ¢┤ļ¢ż ņĢĮņĀ£ņØś ņĪ░ĒĢ®ņØä ņé¼ņÜ®ĒĢĀ Ļ▓āņØĖĻ░ĆņŚÉ ļīĆĒĢ£ ĻĄ¼ņ▓┤ņĀüņØĖ Ļ░ĆņØ┤ļō£ļØ╝ņØĖņØä ņĀ£ņŗ£ĒĢĀ ĒĢäņÜöĻ░Ć ņ׳Ļ▓Āļŗż.
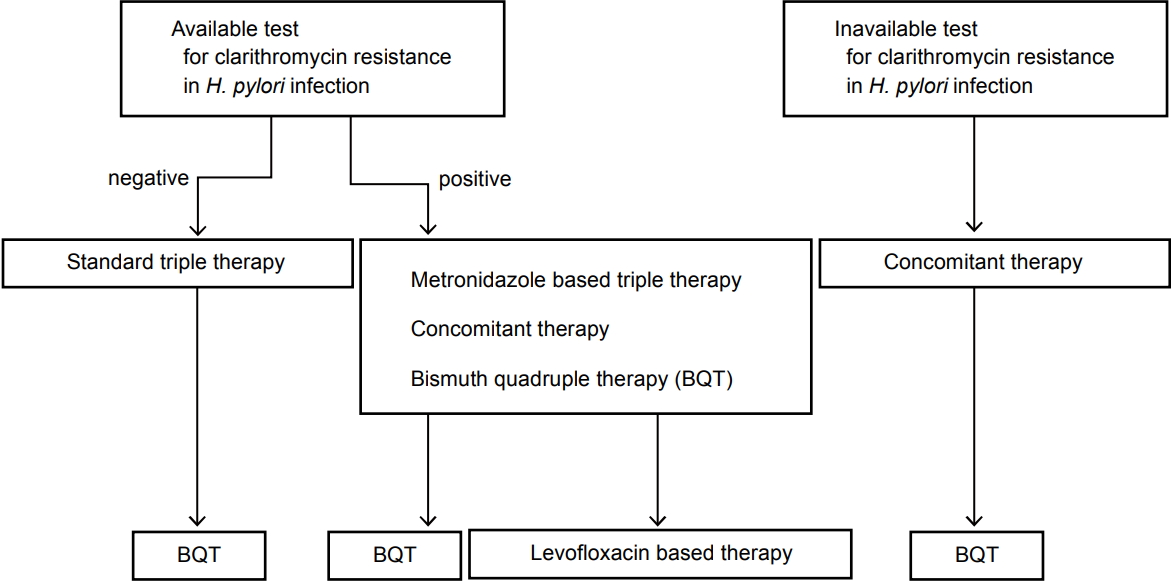
ļÅÖņŗ£ ņ╣śļŻīļŖö PPI, amoxicillin, clarithromycinĻ│╝ metronidazoleņØś 4Ļ░Ćņ¦Ć ņĢĮņĀ£ļź╝ ļÅÖņŗ£ņŚÉ Ēł¼ņĢĮĒĢśļŖö ļ░®ļ▓Ģņ£╝ļĪ£ņä£, Maastricht V/Florence ņ¦äļŻīņ¦Ćņ╣© ļ░Å Toronto ņ¦Ćņ╣©, ļ»ĖĻĄŁ ņåīĒÖöĻĖ░ĒĢÖĒÜī Ļ░ĆņØ┤ļō£ļØ╝ņØĖ ļō▒ņŚÉ ļö░ļź┤ļ®┤ ņØ╝ņ░© ņ╣śļŻīļĪ£ņä£ ņÜ░ņłśĒĢśĻ│Ā, ĒŖ╣Ē׳ clarithromycin ļé┤ņä▒ļźĀņØ┤ ļåÆņØĆ ņ¦ĆņŚŁņŚÉņä£ ņČöņ▓£ļÉĀ ļ¦īĒĢ£ ņ╣śļŻīļĪ£ ņĢīļĀżņĀĖ ņ׳ņ¢┤ņä£ Ļ│ĀļĀżĒĢĀ ņłś ņ׳ļŖö ņ╣śļŻīļ▓ĢņØ┤ļŗż[53-55]. ņØ╝ņ░© ņ╣śļŻīļĪ£ ņä▒Ļ│ĄņĀüņØĖ ņĀ£ĻĘĀ ņ╣śļŻīĻ░Ć ļÉśņ¦Ć ņĢŖņØĆ Ļ▓ĮņÜ░ ņØ┤ņ░© ņ╣śļŻīļĪ£ņä£ bismuth ņé¼ņĀ£ņÜöļ▓Ģ ļ░Å levofloxacin ĻĖ░ļ░śņØś ņé╝ņĀ£ņÜöļ▓ĢņØ┤ Ļ│ĀļĀżļÉĀ ņłś ņ׳ņ£╝ļ®░, ļ╣ĀļźĖ ņŗ£Ļ░ä ļé┤ņŚÉ levofloxacin ĻĖ░ļ░śņØś ņé╝ņĀ£ņÜöļ▓ĢņØ┤ ņé╝ņ░© ņĀ£ĻĘĀ ņÜöļ▓Ģņ£╝ļĪ£ ĻĄŁļé┤ņØś ņÜöņ¢æĻĖēņŚ¼ Ļ│Āņŗ£ņŚÉ ĒżĒĢ©ļÉśņ¢┤ņĢ╝ ĒĢĀ Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż(Fig. 3) [53-55].
Ļ▓░ ļĪĀ
ĻĄŁļé┤ņŚÉņä£ H. pylori ĻĘĀņØś ņĀ£ĻĘĀņ£©ņØ┤ Ļ░ÉņåīĒĢśļŖö ņżæņÜöĒĢ£ ņøÉņØĖņ£╝ļĪ£ clarithromycinņŚÉ ļé┤ņä▒ ņ”ØĻ░Ćļź╝ ņāØĻ░üĒĢĀ ņłś ņ׳ļŗż. ĻĖ░ņĪ┤ņØś ļ░░ņ¢æĻ▓Ćņé¼ļŖö Ļ╣īļŗżļĪ£ņÜ┤ ņĪ░Ļ▒┤Ļ│╝ ņŚ░ĻĄ¼ņ×Éļ¦łļŗż ļŗżļźĖ Ļ▓░Ļ│╝ļź╝ ļ│┤Ļ│ĀĒĢśņŚ¼ ņ×äņāüņŚÉ ņĀüņÜ®ĒĢśĻĖ░ ņ¢┤ļĀżņÜ┤ ļ®┤ņØ┤ ņ׳ņŚłĻ│Ā, ļ░śļ®┤ PCR Ļ▓Ćņé¼ļŖö ļ▓łĻ▒░ļĪ£ņÜ┤ ļ®┤ņØ┤ ņ׳ņŚłļŗż. ņĄ£ĻĘ╝ DPO-PCR Ļ▓Ćņé¼ļŖö ņŚ¼ļ¤¼ ļ▓łņØś Ļ▓Ćņé¼ļź╝ ĒĢ┤ņĢ╝ĒĢĀ ĒĢäņÜöļź╝ ņżäņ×äņ£╝ļĪ£ņŹ© ņŗ£Ļ░äĻ│╝ ļ╣äņÜ®ņØä ļŗ©ņČĢĒĢĀ ņłś ņ׳Ļ▓ī ļÉśņŚłĻ│Ā, ļŹöņÜ▒ņØ┤ ņŗĀņåŹ ņÜöņåīļČäĒĢ┤ĒÜ©ņåī Ļ▓Ćņé¼ļź╝ ĒåĄĒĢ£ DPO-PCR testļŖö PCRņØś ļČłĒÄĖĒĢ©ļÅä ĒĢ┤Ļ▓░ĒĢ┤ ņŻ╝ņŚłļŗż. ĒĢśņ¦Ćļ¦ī ņØ┤ļ¤¼ĒĢ£ ņŗ£ņŖżĒģ£ņØä ĒåĄĒĢśņŚ¼ clarithromycin ļé┤ņä▒ņØä ņÖäņĀäĒ׳ ļŗż ĒīīņĢģĒĢĀ ņłś ņ׳ļŖöĻ░ĆņŚÉ ļīĆĒĢ£ ņØśļ¼ĖņØä Ļ░Ćņ¦ł ņłś ņ׳Ļ│Ā, ņ¢┤ļ¢ż ĒÜ©Ļ│╝ņĀüņØĖ ņĢĮņĀ£ļź╝ ņäĀĒāØĒĢ┤ņĢ╝ ĒĢśļŖöĻ░ĆņŚÉ ļīĆĒĢ£ ļ¼ĖņĀ£ļŖö ņŚ¼ņĀäĒ׳ ļé©ņĢä ņ׳ļŗż. Ē¢źĒøä ņØ┤ļ¤░ ņĀÉļōżņØä ļ│┤ņÖäĒĢśņŚ¼ ņĀ£ĻĘĀ ņĀä ņØ┤ļ¤¼ĒĢ£ ņŗ£ņŖżĒģ£ņØä ņØ┤ņÜ®ĒĢśņŚ¼ ņĀüņĀłĒĢ£ ņĀ£ĻĘĀ ņÜöļ▓ĢņØä ņäĀĒāØĒĢĀ ņłś ņ׳Ļ▓ī ĒĢśņŚ¼ ņØ┤ņāüņĀüņØĖ ņĀ£ĻĘĀņ£©ņØä ņØ┤ļŻ░ ņłś ņ׳ņ¢┤ņĢ╝ ĒĢĀ Ļ▓āņØ┤ļŗż.