ņä£ļĪĀ
ņ£äņĢöņØĆ ņÜ░ļ”¼ļéśļØ╝ņŚÉņä£ Ļ░Ćņן ĒØöĒĢ£ ņĢģņä▒ ņóģņ¢æņ£╝ļĪ£ ņĪ░ņ¦üĒĢÖņĀüņ£╝ļĪ£ ĒØöĒ׳ ņןĒśĢ(intestinal-type)Ļ│╝ ļ»Ėļ¦īĒśĢ(diffuse-type) ņ£äņĢöņ£╝ļĪ£ ļČäļźśĒĢśņŚ¼ ņ¢ĖĻĖēļÉ£ļŗż. ņןĒśĢ ņ£äņĢöņØĆ ņŻ╝ļĪ£ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ (Helicobacter pylori, H. pylori)ņŚÉ ņØśĒĢ┤ ņ£Āļ░£ļÉ£ ļ¦īņä▒ ņ£äņŚ╝ņŚÉņä£ ņ£äņČĢņä▒ ņ£äņŚ╝ ļ░Å ņןņāüĒö╝ĒÖöņāØņØś ņĀäņĢö ņĀÉļ¦ē ļ│ĆĒÖöļź╝ Ļ▒░ņ│É ļ░£ņāØĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŖö ļ░śļ®┤ņŚÉ, ļ»Ėļ¦īĒśĢ ņ£äņĢöņØĆ H. pyloriņŚÉ ņØśĒĢ£ ņ£äņĀÉļ¦ēņØś ĒÖ£ļÅÖņä▒ ņŚ╝ņ”ØņØ┤ ņĀäņĢö ņĀÉļ¦ē ļ│ĆĒÖöļź╝ Ļ▒░ņ╣śņ¦Ć ņĢŖĻ│Ā ļ░£ņāØĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[1-4]. ņןĒśĢ ņ£äņĢöĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ ņĀŖņØĆ ļéśņØ┤ņŚÉ ļ░£ņāØĒĢśĻ│Ā ļé©ļģĆļ╣äņŚÉ ņ░©ņØ┤Ļ░Ć ņŚåĻ▒░ļéś ņŚ¼ņä▒ņŚÉņä£ ļŹö ļ░£ņāØĒĢśļŖö Ļ▓ĮĒ¢źņØ┤ ņ׳Ļ│Ā, ņןĒśĢ ņ£äņĢöņŚÉ ļ╣äĒĢ┤ Ļ│ĄĻ▓®ņĀü ņä▒Ē¢źņØä ļ│┤ņØ┤ļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[5,6]. ņןĒśĢ ņ£äņĢöņØĆ ņÜ░ļ”¼ļéśļØ╝ņÖĆ ņØ╝ļ│ĖĻ│╝ Ļ░ÖņØĆ ļÅÖņĢäņŗ£ņĢäņŚÉņä£ ņÜ░ņäĖĒĢśĻ▓ī ļ░£ņāØĒĢśļéś ļ»Ėļ¦īĒśĢ ņ£äņĢöņØĆ ņןĒśĢ ņ£äņĢöņŚÉ ļ╣äĒĢ┤ ņ¦ĆņŚŁņĀüņ£╝ļĪ£ (geographically) ļŹö ĻĘĀņØ╝ĒĢśĻ▓ī ļČäĒżļÉ£ļŗż[7]. ļ│ĖĻ│ĀņŚÉņä£ļŖö ņØ┤ņÖĆ Ļ░ÖņØ┤ ņןĒśĢĻ│╝ ĻĄ¼ļ│äļÉśļŖö ļ»Ėļ¦īĒśĢ ņ£äņĢöņŚÉ ļīĆĒĢ┤ Ļ▓ĆĒåĀĒĢ┤ļ│┤ļÅäļĪØ ĒĢśĻ▓Āļŗż.
ļ│ĖļĪĀ
1. ļČäļźś
ļ»Ėļ¦īĒśĢ ņ£äņĢöņØĆ ņ£äņĢöņØś ņŚ¼ļ¤¼ ļ│æļ”¼ĒĢÖņĀü ļČäļźś ņ▓┤Ļ│ä ņżæ Lauren ļČäļźśņŚÉ ņØśĒĢ£ļŗż. ņåīĒÖöĻĖ░ļé┤Ļ│╝ ņØśņé¼ņŚÉĻ▓ī ņØĄņłÖĒĢ£ ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ņłĀ ņŗ£ ņĀüņÜ®ļÉśļŖö ļ│æļ”¼ ļČäļźśļ▓ĢņŚÉ ņØśĒĢ£ ļ»ĖļČäĒÖöĒśĢ(undifferentiated-type) ņ£äņĢöņØś ļīĆļČĆļČäņØ┤ ļ»Ėļ¦īĒśĢ ņ£äņĢöņŚÉ ĒĢ┤ļŗ╣ļÉ£ļŗż. ņØ╝ļ│ĖņØś ļČäļźśļĪ£ļŖö signet-ring cell carcinoma (sig)ņÖĆ poorly differentiated adenocarcinoma (por) ņżæ non-solid ĒśĢĒā£(por2)Ļ░Ć ļ»Ėļ¦īĒśĢ ņ£äņĢöņŚÉ ņåŹĒĢśļ®░, World health Organization (WHO) 2019 ļČäļźś ņ▓┤Ļ│äļĪ£ļŖö poorly cohesive type (signet-ring cell phenotype, other cell types)ņØ┤ ļ»Ėļ¦īĒśĢ ņ£äņĢöņŚÉ ņåŹĒĢ£ļŗż(Table 1).
SigņÖĆ por2Ļ░Ć ļ»Ėļ¦īĒśĢ ļ░Å ļ»ĖļČäĒÖöĒśĢ ņ£äņĢöņ£╝ļĪ£ Ļ░ÖņØ┤ ļČäļźśļÉśĻ│Ā ņ׳ņ£╝ļéś ņŗżņĀ£ ņāØļ¼╝ĒĢÖņĀü Ē¢ēĒā£(biologic behavior) ņĖĪļ®┤ņŚÉņä£ ļÅÖņØ╝ĒĢśĻ▓ī ļČäļźśĒĢśļŖö Ļ▓āņØ┤ ļ¦×ļŖöņ¦ĆņŚÉ ļīĆĒĢ┤ņä£ļŖö ņóĆ ļŹö Ļ▓Ćņ”ØņØ┤ ĒĢäņÜöĒĢĀ ņłś ņ׳ļŗż. ņ£äņĢöņØ┤ ņ¦äĒ¢ēĒĢśļ®┤ņä£ ĒśĢĒā£ĒĢÖņĀü ļČäĒÖöĻ░Ć ņĀĆļČäĒÖöļĪ£ ļ│ĆĒÖöĒĢĀņłś ņ׳ĻĖ░ ļĢīļ¼ĖņŚÉ sigņÖĆ por2ņØś ņāØļ¼╝ĒĢÖņĀü Ē¢ēĒā£ņØś ņ░©ņØ┤ļŖö ņĪ░ĻĖ░ņ£äņĢöņŚÉņä£ ņ░©ņØ┤ļź╝ ļ│┤ņØ╝ ņłś ņ׳ļŗż. ņŗżņĀ£ ņĪ░ĻĖ░ņ£äņĢö Ļ┤ĆļĀ© ņŚ░ĻĄ¼ļōżņŚÉņä£ sig ļ░Å por2 Ļ░äņŚÉ ņ░©ņØ┤ļź╝ ļ│┤ņ×äņØä ļ│┤Ļ│ĀĒĢśĻ│Ā ņ׳ļŖöļŹ░ ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ Ēøä ņĄ£ņóģ ļ│æļ”¼ Ļ▓░Ļ│╝ņŚÉņä£ sigņØś Ļ▓ĮņÜ░ļŖö ņłśĒÅēņĀłņĀ£ņŚ░ ņ╣©ļ▓öņØ┤ ņ¢æņä▒ņØĖ Ļ▓ĮņÜ░Ļ░Ć, porņØś Ļ▓ĮņÜ░ļŖö ņłśņ¦üņĀłņĀ£ņŚ░ ņ╣©ļ▓öņØ┤ ņ¢æņä▒ņØĖ Ļ▓ĮņÜ░Ļ░Ć ņāüļīĆņĀüņ£╝ļĪ£ ļ╣łļ▓łĒĢśņśĆļŗż[8-11]. ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ļŖö ļČłņÖäņĀä ņĀłņĀ£ ņżæ Ļ░Ćņן ĒØöĒĢ£ ņØ┤ņ£ĀĻ░Ć porņØś Ļ▓ĮņÜ░ļŖö ņłśņ¦üņĀłņĀ£ņŚ░ ņ╣©ļ▓ö ņ¢æņä▒(51.1%)ņØ┤ņŚłĻ│Ā, sigņØś Ļ▓ĮņÜ░ļŖö ņłśĒÅēņĀłņĀ£ņŚ░ ņ╣©ļ▓ö ņ¢æņä▒(63.3%)ņ£╝ļĪ£ ļ│┤Ļ│ĀĒĢśņśĆņ£╝ļ®░, ĻĄŁļé┤ ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ ļĀłņ¦ĆņŖżĒŖĖļ”¼ ļČäņäØ Ļ▓░Ļ│╝ņŚÉņä£ļÅä ļČłņÖäņĀä ņĀłņĀ£ņØś Ļ▓ĮņÜ░ ņłśņ¦üņĀłņĀ£ņŚ░ ņ╣©ļ▓ö ņ¢æņä▒ņØ┤ por, sig Ļ░üĻ░ü 60.0%, 25.0%, ņłśĒÅēņĀłņĀ£ņŚ░ ņ╣©ļ▓ö ņ¢æņä▒ņØĆ por, sig Ļ░üĻ░ü 26.7%, 50.0%ļĪ£ ļ│┤Ļ│ĀĒĢśņśĆ ļŗż[8-11]. ļśÉĒĢ£, ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ļŖö porĻ│╝ sigņØś 1,295Ļ░£ņØś ņłśņłĀ ļ│æļ│ĆĻ│╝ 176Ļ░£ņØś ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ ļ│æļ│ĆņØä ļ╣äĻĄÉĒĢśņśĆņØä ļĢī ļ»Ėļ¦īĒśĢņ£╝ļĪ£ Ļ░ÖņØ┤ ļČäļźśļÉśĻ│Ā ņ׳ļŖö sigņÖĆ por2Ļ░Ć ļ”╝ĒöäņĀł ņĀäņØ┤ ļ░Å ļ”╝ĒöäĒśłĻ┤Ćņ╣©ļ▓öĻ│╝ Ļ░ÖņØĆ ņāØļ¼╝ĒĢÖņĀü Ē¢ēĒā£ņŚÉņä£ ņ░©ņØ┤ļź╝ ļ│┤ņśĆņ£╝ļ®░, ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ ņØ┤Ēøä ņĀłņĀ£ņŚ░ ņ¢æņä▒ņŚÉ ņ׳ņ¢┤ņä£ļÅä ņ░©ņØ┤ļź╝ ļ│┤ņśĆļŗż[10].
ņØ┤ņÖĆ Ļ░ÖņØĆ ņŚ¼ļ¤¼ Ļ▓░Ļ│╝ļōżņØ┤ 2010ļģä WHO classificationņŚÉņä£ poorly cohesive carcinoma ĒĢśļéśļĪ£ ļČäļźśĒĢ£ Ļ▓āņØä 2019ļģäņŚÉ ļ░£Ēæ£ļÉ£ Ļ░£ņĀĢĒīÉņŚÉņä£ļŖö poorly cohesive carcinoma ļé┤ņŚÉņä£ sig ĒśĢĒā£ņÖĆ ļŗżļźĖ ĒśĢĒā£ļĪ£ ļČäļźśĒĢ£ ņØ┤ņ£ĀņØ╝ Ļ▓āņØ┤ļŗż. ņØ┤ņÖĆ Ļ░ÖņØĆ ņ░©ņØ┤ļź╝ ļ│┤ņØ┤ļŖö ņøÉņØĖ ņżæ ĒĢśļéśļŖö sigņÖĆ porņØś ņĢöņäĖĒż ņä▒ņן Ēī©Ēä┤(growth pattern)ņØś ņ░©ņØ┤ļĪ£, ņĪ░ĻĖ░ņØś sigņØś Ļ▓ĮņÜ░ ņĢöņäĖĒżņØś ņä▒ņן Ēī©Ēä┤ņØ┤ ņĖĪļ░®ĒśĢņØ┤ ņÜ░ņäĖĒĢśĻ│Ā, porņØś Ļ▓ĮņÜ░ļŖö ņłśņ¦üĒśĢņØ┤ ņÜ░ņäĖĒĢśĻĖ░ ļĢīļ¼Ėņ£╝ļĪ£ ņČöņĖĪļÉ£ļŗż. ņŗżņĀ£ ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ļŖö sigņŚÉņä£ ņŻ╝ļ│Ć ņĀÉļ¦ēņØ┤ ņ£äņČĢņä▒ ņ£äņŚ╝ņØ┤ļéś ņןņāüĒö╝ ĒÖöņāØĻ│╝ Ļ░ÖņØ┤ mechanical barrierĻ░Ć ņĢĮĒĢ┤ņĀĖ ņ׳ļŖö ļ¦īņä▒ ņĀÉļ¦ē ļ│ĆĒÖöĻ░Ć ļÅÖļ░śļÉśļŖö Ļ▓ĮņÜ░ ņĖĪļ░®ĒśĢ ņä▒ņן Ēī©Ēä┤ņØ┤ ļŹö ļæÉļō£ļ¤¼ņ¦ĆĻ▓ī ļéśĒāĆļé©ņØä ļ│┤Ļ│ĀĒĢśņśĆļŗż[12,13].
Next generation sequencing, RNA sequencing, Whole genome sequencing ļ░®ļ▓Ģņ£╝ļĪ£ ņ£äņĢöņØś ļČäņ×ÉņāØļ¼╝ĒĢÖņĀü ļČäļźśĻ░Ć Ļ░ĆļŖźĒĢ┤ņĪīĻ│Ā, ņĢö Ļ▓īļåł ņĢäĒŗĆļØ╝ņŖż (The Cancer Genome Altas, TCGA) ņŚ░ĻĄ¼ ļ░Å Asian Cancer Research Group (ACRG) cohortņŚÉņä£ ņ£äņĢöņØś ļČäņ×ÉņāØļ¼╝ĒĢÖņĀü ļČäļźśļź╝ ņĀ£ņŗ£ĒĢśņśĆļŗż[14-16]. TCGA ņŚÉņä£ļŖö ņ£äņĢöņØä 4Ļ░£ņØś ļČäņ×É ĒĢśņ£ä ņ£ĀĒśĢ ņ”ē, EBV ņ¢æņä▒, microsatellite unstable, genomically stable (GS), chromosomal instabilityļĪ£ ļČäļźśĒĢśņśĆĻ│Ā, ņØ┤ ņżæ ļ»Ėļ¦īĒśĢ ņ£äņĢöņØś ļīĆļČĆļČäņØĖ ņĢĮ 73%Ļ░Ć GSļĪ£ ļČäļźśļÉśņŚłļŗż. GS ļé┤ņŚÉņä£ ļåÆĻ▓ī Ļ┤Ćņ░░ļÉ£ ņ▓┤ņäĖĒż ļÅīņŚ░ļ│ĆņØ┤ļŖö CDH1 ļÅīņŚ░ļ│ĆņØ┤Ļ░Ć ņĢĮ 37%, RHOA ļÅīņŚ░ļ│ĆņØ┤Ļ░Ć ņĢĮ 15%, CLDN18-ARHGAP ņ£ĄĒĢ®(fusion)ņØ┤ ņĢĮ 15%ņŚÉņä£ Ļ┤Ćņ░░ļÉśņŚłļŗż. ĒĢ£ņŚ░ĻĄ¼ņŚÉņä£ TCGA ļČäļźśļź╝ ĻĖ░ļ░śņ£╝ļĪ£ ņśłņĖĪļ¬©ļŹĖņØä ļ¦īļōżĻ│Ā ļæÉ Ļ░£ņØś ļīĆĻĘ£ļ¬© ņĮöĒśĖĒŖĖļĪ£ Ļ▓Ćņ”ØĒĢśņśĆņØä ļĢī GS cohortĻ░Ć ņłśņłĀ Ēøä ļ│┤ņĪ░ĒĢŁņĢöņÜöļ▓Ģ ņØ┤Ēøä ņ×¼ļ░£ļźĀņØ┤ ļåÆĻ│Ā ņśłĒøäĻ░Ć ļéśņü©ņØä ļ│┤Ļ│ĀĒĢśņśĆļŗż[15].
ACRGņŚÉņä£ļÅä ņ£äņĢöņØä 4Ļ░£ņØś ņĢäĒśĢņ£╝ļĪ£ ļČäļźśĒĢśņśĆļŗż[16]. Ļ░Ćņן ņóŗņØĆ ņśłĒøäļź╝ ļ│┤ņØ┤ļŖö microsatellite unstableĻĄ░ ļ░Å 3Ļ░£ņØś microsatellite stable (MSS)ĻĄ░ ņ”ē, MSS/TP53-ĒÖ£ņä▒, MSS/TP53-ļ╣äĒÖ£ņä▒ ļ░Å MSS/epithelial to mesenchymal transition (EMT)ĻĄ░ņ£╝ļĪ£ ļČäļźśĒĢśņśĆļŗż[16]. ņØ┤ ņżæ TCGAņØś GSņÖĆ Ļ░Ćņן ņ£Āņé¼ĒĢ£ ĻĄ░ņØĆ MSS/EMTĻĄ░ņ£╝ļĪ£ 80% ņØ┤ņāüņØ┤ ļ»Ėļ¦īĒśĢ ņ£äņĢöņ£╝ļĪ£, CDH1 ņåīņŗż, Ļ░Ćņן ļČłļ¤ēĒĢ£ ņśłĒøä, ņ¦äļŗ© ļŗ╣ņŗ£ ņ¦äĒ¢ēņä▒ ļŗ©Ļ│ä, ļåÆņØĆ ņ×¼ļ░£ļźĀ, ļ│Ąļ¦ē ņĀäņØ┤ņØś ĒŖ╣ņä▒ņØä ļ│┤ņśĆļŗż. ļśÉĒĢ£ ļÅīņŚ░ļ│ĆņØ┤ ļ░£ņāØļźĀņØ┤ ļŗżļźĖ ĻĄ░ņŚÉ ļ╣äĒĢ┤ ļé«ņĢśļŗż. ņØ┤ļŖö ļ»Ėļ¦īĒśĢ ņ£äņĢöņŚÉņä£ ņĢöĒÖö Ļ│╝ņĀĢ ĻĘ£ļ¬ģ ļ░Å ņ╣śļŻīņĀ£ Ļ░£ļ░£ņØä ņ£äĒĢ£ driver gene ļ░£ĻĄ┤ņØ┤ ņ¢┤ļĀżņøĆņØä ņŗ£ņé¼ĒĢ£ļŗż.
2. ļ│æĒā£ņāØļ”¼
ņןĒśĢ ņ£äņĢö ļ░£ņāØņŚÉ ņ׳ņ¢┤ņä£ļŖö H. pylori Ļ░ÉņŚ╝Ļ│╝ ĒĢ©Ļ╗ś ņżæņÜöĒĢśĻ▓ī ņ¢ĖĻĖēļÉśļŖö correa cascade ļ░Å ņŚ¼ļ¤¼ ņ£ĀņĀäņĀü ņÜöņØĖ, ĒÖśĻ▓ĮņĀü ņÜöņØĖ ļō▒ņØ┤ Ļ┤ĆņŚ¼ļÉ£ļŗżĻ│Ā ņĢīļĀżņĀĖ ņ׳ļŗż[17]. ĒĢśņ¦Ćļ¦ī ņןĒśĢ ņ£äņĢö ļ░£ņāØņŚÉņä£ ņżæņÜöĒĢśĻ▓ī ņ¢ĖĻĖēļÉśļŖö ĒÖśĻ▓Į ņÜöņØĖ ļ░Å ļ¦īņä▒ ņŚ╝ņ”Ø cascadeļŖö ļ»Ėļ¦īĒśĢ ņ£äņĢö ļ░£ņāØņŚÉņä£ļŖö ļŹ£ Ļ┤ĆņŚ¼ĒĢ£ļŗżĻ│Ā ņĢīļĀżņĀĖ ņ׳ļŗż. ņ”ē, ļ»Ėļ¦īĒśĢ ņ£äņĢö ļ░£ņāØņŚÉ ņ׳ņ¢┤ņä£ ņ£ĀņĀäņĀü ņåīņØĖņØ┤ ņżæņÜöĒĢĀ Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉśņ¦Ćļ¦ī ņ£äņĢöņØś ļČäņ×ÉņāØļ¼╝ĒĢÖņĀü ļČäļźśņŚÉņä£ļÅä ņĢī ņłś ņ׳ļō»ņØ┤ ļ»Ėļ¦īĒśĢ ņ£äņĢöĒÖö Ļ│╝ņĀĢņØś ĻĘ╝ļ│ĖņĀüņØĖ ļČäņ×É Ļ▓ĮļĪ£ļŖö ņĢäņ¦ü ņל ĻĘ£ļ¬ģļÉśņ¦Ć ņĢŖņĢśļŗż. ĻĘĖļ¤╝ņŚÉļÅä ņØ┤ņĀä ņ£äņĢöņØś ļČäņ×ÉņĀü ļ│æĒā£ ņāØļ”¼ļź╝ ņÜöņĢĮĒĢ£ ļ│┤Ļ│Āļź╝ ļ░öĒāĢņ£╝ļĪ£ ļ»Ėļ¦īĒśĢ ņ£äņĢö ļ░£ņāØņŚÉ Ļ┤ĆņŚ¼ĒĢśļŖö ļČäņ×É ņāØļ¼╝ĒĢÖņĀü ņÜöņåīļōżņØä ņĀĢļ”¼ĒĢ┤ļ│┤ļ®┤ Table 2ņÖĆ Ļ░Öļŗż[17-26]. ņ”ē, ļ»Ėļ¦īĒśĢ ņ£äņĢö ļ░£ņāØņŚÉņä£ Ļ░Ćņן ņżæņÜöĒĢ£ Ēśäņāü ņżæ ĒĢśļéśņØĖ ņäĖĒżĻ░ä ņĀæņ┤ēĻ│╝ Ļ┤ĆļĀ©ļÉ£ E-cadherinĻ│╝ Ļ┤ĆļĀ©ļÉ£ ņ£ĀņĀäņ×É ļ░Å ļČäņ×É Ļ▓ĮļĪ£, H. pyloriņÖĆ Ļ┤ĆļĀ©ļÉ£ ĻĖ░ņĀäļōżņØ┤ļŗż.
3. ļé┤ņŗ£Ļ▓Į ņ¦äļŗ©
ņ£äņĢöņØś ņ¦äļŗ©ņŚÉ ņ׳ņ¢┤ņä£ Ļ░Ćņן ņżæņÜöĒĢ£ Ļ▓āņØĆ ļé┤ņŗ£Ļ▓Į ņåīĻ▓¼ņØ┤ļŗż. ļ»Ėļ¦īĒśĢ ņ£äņĢöņØ┤ ņןĒśĢ ņ£äņĢöņŚÉ ļ╣äĒĢ┤ ņāØļ¼╝ĒĢÖņĀü Ē¢ēĒā£Ļ░Ć Ļ│ĄĻ▓®ņĀüņØ┤Ļ│Ā ņśłĒøäĻ░Ć ļČłļ¤ēĒĢśļŗżĻ│Ā ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ņ¦Ćļ¦ī ņĪ░ĻĖ░ņŚÉ ņ¦äļŗ©ļÉĀ Ļ▓ĮņÜ░ ņśłĒøäļŖö ņ¢æĒśĖĒĢśļŗż. ļ»Ėļ¦īĒśĢ ņ£äņĢö ņżæ sigņØś Ļ▓ĮņÜ░ļŖö ļ¦ÄņØĆ ņŚ░ĻĄ¼ņŚÉņä£ ņĪ░ĻĖ░ ņ¦äļŗ© ņŗ£ ļ”╝ĒöäņĀł ņĀäņØ┤Ļ░Ć ņśżĒ׳ļĀż ļé«Ļ│Ā ņśłĒøäļÅä ņóŗļŗżĻ│Ā ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ļŗż[27-30]. ļö░ļØ╝ņä£, ļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ļź╝ ĒåĄĒĢ£ ņĪ░ĻĖ░ ņ¦äļŗ©ņØ┤ ļ¦żņÜ░ ņżæņÜöĒĢśļŗż.
ņĪ░ĻĖ░ņ£äņĢöņØś ļČäĒÖöļÅäņŚÉ ļö░ļźĖ ļé┤ņŗ£Ļ▓Į ņåīĻ▓¼ņØä ļČäņäØĒĢ£ ņŚ░ĻĄ¼ļź╝ ļ│┤ļ®┤ ņ£ĄĻĖ░ĒśĢ(I, IIa)ņØĆ ņןĒśĢ ņ£äņĢöņŚÉņä£ Ļ░Ćņן ļ¦ÄņØ┤ Ļ┤Ćņ░░ļÉśņŚłĻ│Ā, ĒÄĖĒÅēĒśĢ(IIb)ņØĆ ļ»Ėļ¦īĒśĢ ņ£äņĢö ņżæņŚÉņä£ļÅä sigņŚÉņä£ Ļ░Ćņן ĒØöĒĢśĻ▓ī Ļ┤Ćņ░░ļÉśņŚłļŗż[31]. ĒÄĖĒÅēĒśĢņØĆ ņ£ĄĻĖ░ļéś ĒĢ©ļ¬░ņØ┤ ļÅÖļ░śļÉśņ¦Ć ņĢŖņØĆ ņāēņĪ░ ļ│ĆĒÖöņØ┤ĻĖ░ ļĢīļ¼ĖņŚÉ ļŹö ļ®┤ļ░ĆĒĢ£ Ļ┤Ćņ░░ņØ┤ ņÜöĻĄ¼ļÉ£ļŗż. ļö░ļØ╝ņä£ ļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ ņŗ£ ļ»Ėļ¦īĒśĢ ņĪ░ĻĖ░ņ£äņĢöņØś ņĪ░ĻĖ░ ņ¦äļŗ©ņØä ņ£äĒĢ┤ ņāēņĪ░ ļ│ĆĒÖöĻ╣īņ¦Ć Ļ╝╝Ļ╝╝Ē׳ ņé┤Ēö╝ļŖö Ļ▓āņØ┤ ņżæņÜöĒĢśĻ▓Āļŗż. Fig. 1ņØĆ ĒÄĖĒÅēĒśĢņ£╝ļĪ£ ņ¦äļŗ©ļÉ£ ļ»Ėļ¦īĒśĢ ņĪ░ĻĖ░ņ£äņĢöņØś ļé┤ņŗ£Ļ▓Į ņåīĻ▓¼ļōżņØ┤ļŗż. ļ│æļ│ĆņØś ņāēņĪ░ ļ│ĆĒÖöļź╝ Ļ╝╝Ļ╝╝Ē׳ Ļ▓ĆĒåĀĒĢśļŖö Ļ▓āņØĆ ļ│æļ│Ć ņ¦äļŗ©ļ┐Éļ¦ī ņĢäļŗłļØ╝ ļ│æļ│ĆņØś Ļ▓ĮĻ│äļź╝ ļ¬ģĒÖĢĒ׳ ĒÅēĻ░ĆĒĢśļŖö Ļ▓āņŚÉļÅä ņżæņÜöĒĢśļŗż.
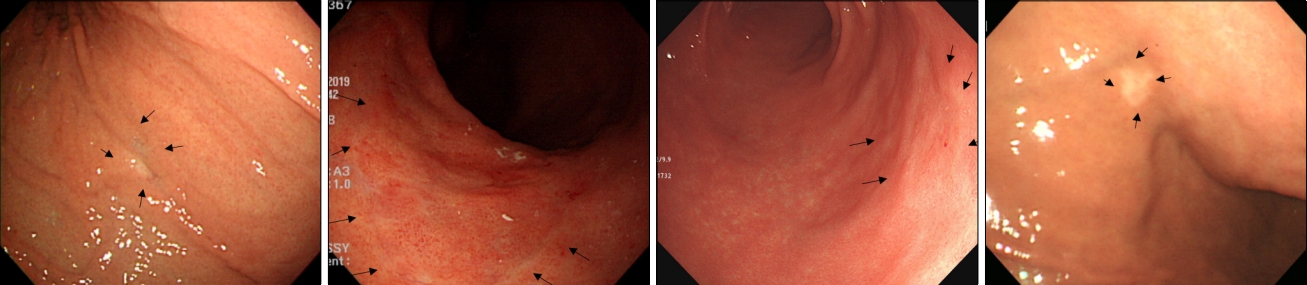
ļśÉĒĢ£ ļ»Ėļ¦īĒśĢ ņ£äņĢöņØś ļé┤ņŗ£Ļ▓Į ņåīĻ▓¼ņŚÉņä£ ņżæņÜöĒĢ£ Ļ▓āņØĆ ņ¦äĒ¢ēĒśĢ ņ£äņĢö ņżæ ļ│┤ļ¦ī 4ĒśĢņØ┤ļŗż. ļ│┤ļ¦ī 4ĒśĢņØś ļé┤ņŗ£Ļ▓Į ņåīĻ▓¼ņØ┤ ļ»Ėļ¦īĒśĢ ņ£äņĢöņØś ļīĆĒæ£ņĀü ĒŖ╣ņ¦Ģ ņżæ ĒĢśļéśņ×äņØĆ ņל ņĢīļĀżņĀĖ ņ׳ļŗż. ņØ┤ ņåīĻ▓¼ņØ┤ ņżæņÜöĒĢ£ ņØ┤ņ£ĀļŖö ņØ╝ļ░śņĀüņØĖ ļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ņŚÉņä£ ņ£ĪņĢłņĀüņ£╝ļĪ£ ĒŖ╣ņ¦ĢņĀü ļ│æļ│ĆņØ┤ ņŚåņ¢┤ņä£ Ļ░äĻ│╝ļÉśĻĖ░ ņēĮĻĖ░ ļĢīļ¼ĖņØ┤ļŗż. ņĀÉļ¦ē ļ│ĆĒÖö ņŚåļŖö ņĢöņäĖĒż ņĀÉļ¦ēĒĢś ņ╣©ņ£żņ£╝ļĪ£ ņĪ░ņ¦ü Ļ▓Ćņé¼ņŚÉņä£ ņ£äņØīņä▒ņØ┤ ļ¦ÄĻĖ░ ļĢīļ¼ĖņŚÉ ņ¦äļŗ©ņĀü ņĖĪļ®┤ņŚÉņä£ ļ¦żņÜ░ ņżæņÜöĒĢ£ ļé┤ņŗ£Ļ▓Į ņåīĻ▓¼ņØ┤ļŗż. ļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ ņŗ£ Ļ│ĄĻĖ░ ņŻ╝ņ×ģņŚÉļÅä ņ£äĻ░Ć ņל ņŗĀņĀäļÉśņ¦Ć ņĢŖĻ│Ā ņŻ╝ļ”äņØ┤ ļ╣äĒøä ļÉśņ¢┤ņ׳ļŖö Ļ▓āņØ┤ Ļ░Ćņן ĒŖ╣ņ¦ĢņĀüņØĖ ņåīĻ▓¼ņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż. ļ»Ėļ×Ćņä▒ ĒĢ©ļ¬░ ļō▒ ņĀÉļ¦ē ļ│ĆĒÖöĻ░Ć ļÅÖļ░śļÉśļŖö Ļ▓ĮņÜ░Ļ░Ć ņ׳ļŖöļŹ░, ņĪ░ņ¦ü Ļ▓Ćņé¼ļŖö ņĀÉļ¦ē ļ│ĆĒÖöĻ░Ć ļÅÖļ░śļÉ£ ļČĆņ£äņŚÉņä£ ĒĢśļŖö Ļ▓āņØ┤ ņ¦äļŗ©ņØä ļåÆņØ╝ ņłś ņ׳ļŗż. Fig. 2ļŖö ļ»Ėļ¦īĒśĢ ņ£äņĢöņØś ļ│┤ļ¦ī 4ĒśĢ ļé┤ņŗ£Ļ▓Į ņåīĻ▓¼ļōżņØ┤ļŗż. ļ░śļ│ĄņĀü ņāØĻ▓Ć, ņĀÉļ¦ēļ░Ģļ”¼ņłĀĻ│╝ ĒĢ©Ļ╗ś ņĀłņĀ£ļ®┤ ņāØĻ▓Ć ļō▒ ņĀüĻĘ╣ņĀü Ļ▓Ćņé¼ļź╝ ĒåĄĒĢ£ ņ¦äļŗ©ņØ┤ ņĢłļÉśļŹöļØ╝ļÅä ļé┤ņŗ£Ļ▓Į ņåīĻ▓¼ņØ┤ Ļ░ĢļĀźĒĢśĻ▓ī ņØśņŗ¼ļÉĀ Ļ▓ĮņÜ░ņŚÉļŖö ņłśņłĀņĀü ĒÖĢņ¦ä ļ░Å ņ╣śļŻīļź╝ ļÅÖņŗ£ņŚÉ ņŗ£Ē¢ēĒĢśņŚ¼ņĢ╝ ĒĢ£ļŗż.
4. ņ╣śļŻī
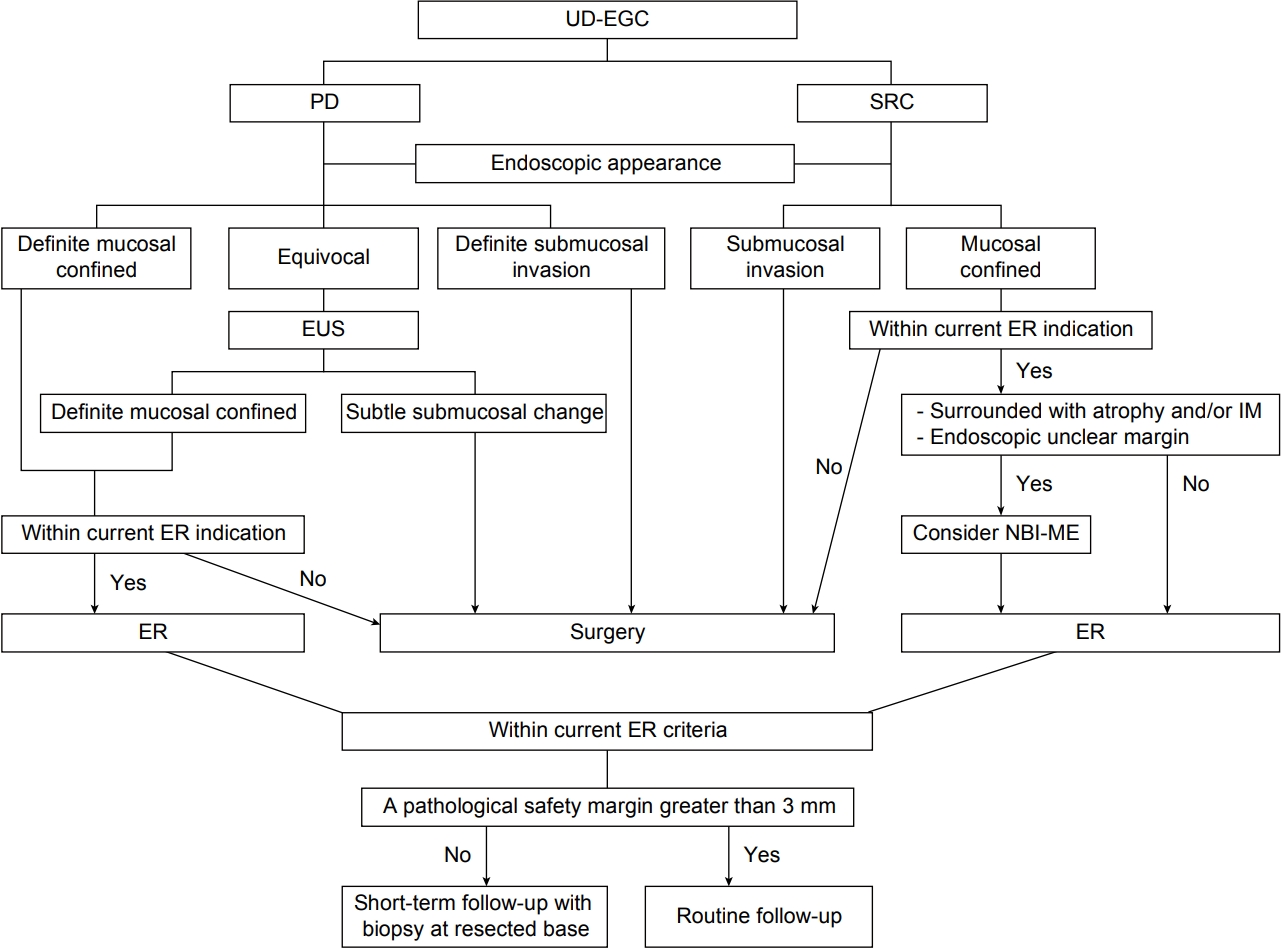
ļ»Ėļ¦īĒśĢ ņĪ░ĻĖ░ņ£äņĢö ņ╣śļŻīņŚÉ ņ׳ņ¢┤ņä£ ļé┤ņŗ£Ļ▓ĮņĀü ņĀłņĀ£ņłĀņØĆ 2 cm ņØ┤ĒĢśņØś ĻČżņ¢æņØä ļÅÖļ░śĒĢśņ¦Ć ņĢŖļŖö ņĀÉļ¦ēņĢöņØś Ļ▓ĮņÜ░ņŚÉ ņŗ£Ē¢ēļÉĀ ņłś ņ׳ļŗż. ņØ┤ Ļ▓ĮņÜ░ ņ£äņĢöņØś Ēæ£ņżĆ ņ╣śļŻīļŖö ņ£ä ņĀłņĀ£ņłĀņØ┤ļ®░ ļé┤ņŗ£Ļ▓ĮņĀłņĀ£ņłĀņØĆ ņĢäņ¦üĻ╣īņ¦Ć ņŗ£ĒŚśņĀü ņ╣śļŻīņŚÉ ĒĢ┤ļŗ╣ļÉśņ¦Ćļ¦ī[32,33], Ēśäņ×¼ ņ¦äĒ¢ēļÉśĻ│Ā ņ׳ļŖö ļ»ĖļČäĒÖöĒśĢ ņĪ░ĻĖ░ņ£äņĢöņŚÉņä£ ņłśņłĀĻ│╝ ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ņłĀņŚÉ ļīĆĒĢ£ ĻĄŁļé┤ ņĀäĒ¢źņĀü ļŗżĻĖ░Ļ┤Ć ņŚ░ĻĄ¼(ClinicalTrial.gov: NCT04890171, CRIS: KCT0006159) Ļ▓░Ļ│╝ļź╝ ĒåĄĒĢ┤ ņ╣śļŻī ņĀäļץņØ┤ ĒÖĢļ”ĮļÉĀ Ļ▓āņ£╝ļĪ£ ĻĖ░ļīĆĒĢ£ ļŗż. ĻĘĖļÅÖņĢł ļ│┤Ļ│ĀļÉ£ ļīĆļČĆļČäņØś ņŚ░ĻĄ¼ļōżņØ┤ ĒøäĒ¢źņĀü ļČäņäØņØ┤Ļ│Ā ņØ╝ļ│ĖņŚÉņä£ ļ│┤Ļ│ĀĒĢ£ ļ»ĖļČäĒÖöĒśĢ ņĪ░ĻĖ░ņ£äņĢöņØś ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ņłĀņŚÉ ļīĆĒĢ£ ļŗżĻĖ░Ļ┤Ć ņĀäĒ¢źņĀü Ļ┤Ćņ░░ ņŚ░ĻĄ¼ļÅä ņłśņłĀĻ│╝ņØś ļ╣äĻĄÉĻ░Ć ņĢäļŗī ļŗ©ņØ╝ĻĄ░ ņŚ░ĻĄ¼ļØ╝ļŖö ĒĢ£Ļ│äĻ░Ć ņ׳ĻĖ┤ ĒĢśņ¦Ćļ¦ī, ĻĖ░ņĪ┤ņØś ņŚ░ĻĄ¼ļōżņØä ļ│╝ ļĢī Ēśäņ×¼Ļ╣īņ¦Ć ļ│┤Ļ│ĀļÉ£ ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ņłĀ ņĀüņØæņ”Ø ļé┤ņŚÉņä£ ĻĘ╝ņ╣śņĀü ņĀłņĀ£Ļ░Ć ņØ┤ļŻ©ņ¢┤ņ¦ä Ļ▓ĮņÜ░ ņśłĒøäļŖö ņ¢æĒśĖĒĢ£ Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ļŗż[8,9,34-38]. ĒĢśņ¦Ćļ¦ī, ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ņłĀ ĻĖ░ņżĆņØś ļČäĒÖöĒśĢ ņĪ░ĻĖ░ņ£äņĢöņŚÉ ĒĢ┤ļŗ╣ĒĢśļŖö ņןĒśĢ ņĪ░ĻĖ░ņ£äņĢöĻ│╝ ļ╣äĻĄÉĒĢĀļĢī ĻĘ╝ņ╣ś ņĀłņĀ£ņ£©ņØ┤ ņāüļīĆņĀüņ£╝ļĪ£ ļé«ņØĆ Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│ĀļÉ£ļŗż[9]. ļö░ļØ╝ņä£ ļ»ĖļČäĒÖöĒśĢ ņĪ░ĻĖ░ņ£äņĢöņŚÉņä£ ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ļź╝ ņŗ£Ē¢ēĒĢĀ ļĢī ĻĘ╝ņ╣śņĀłņĀ£Ļ░Ć ņØ┤ļŻ©ņ¢┤ņ¦ĆļŖö ņĀäļץņØ┤ ņżæņÜöĒĢĀ ņłś ņ׳ļŗż[5,39].
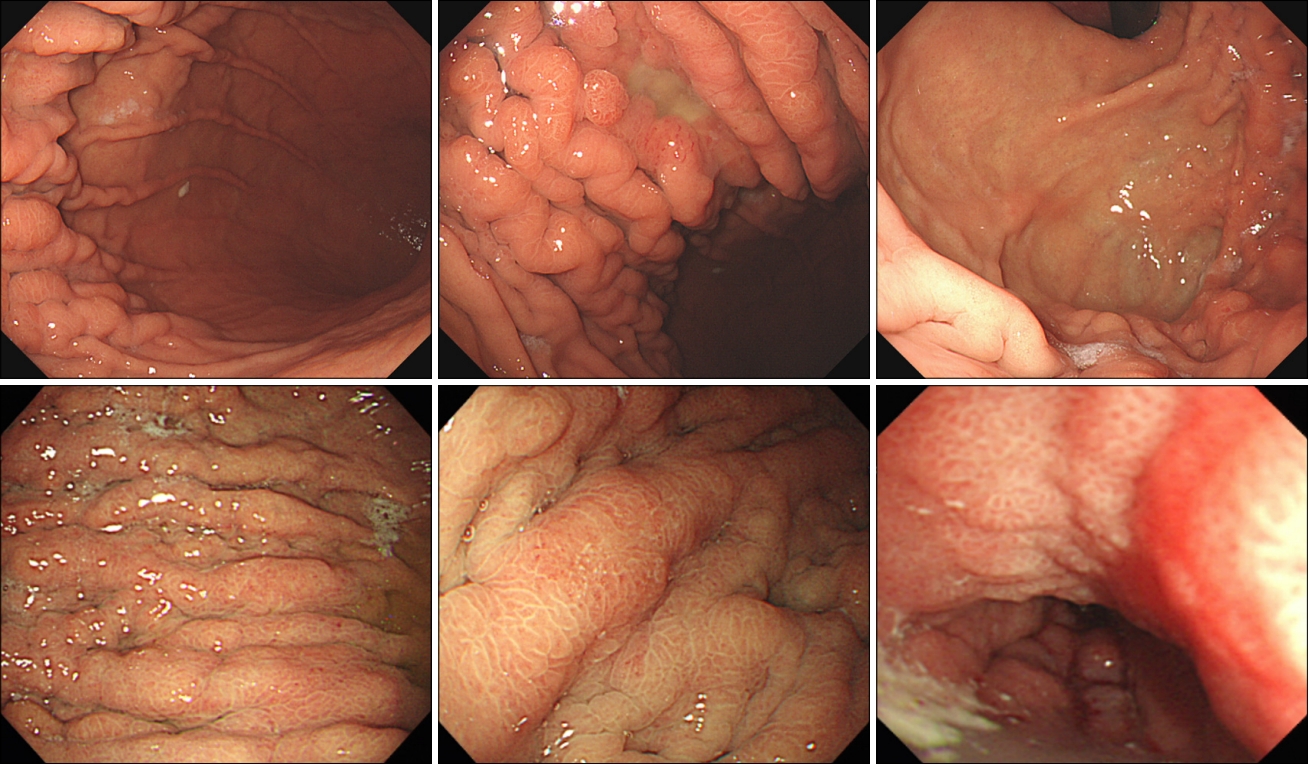
ļ»ĖļČäĒÖöĒśĢ ņĪ░ĻĖ░ņ£äņĢöņŚÉņä£ ĻĘ╝ņ╣śņĀü ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ņłĀņØ┤ ļÉśĻĖ░ ņ£äĒĢ┤ņä£ļŖö Ļ░ü ņäĖĒż ĒśĢĒā£ņŚÉ ļö░ļźĖ ņāØļ¼╝ĒĢÖņĀü Ē¢ēĒā£ļź╝ Ļ│ĀļĀżĒĢ£ ņĀæĻĘ╝ņØ┤ ĒĢäņÜöĒĢĀ ņłś ņ׳ļŗż. ņ£äņŚÉ ņ¢ĖĻĖēĒĢ£ļīĆļĪ£ sigņÖĆ porņØĆ ņä▒ņן Ēī©Ēä┤ņØ┤ ļŗżļź┤ĻĖ░ ļĢīļ¼ĖņŚÉ ņØ┤ļź╝ Ļ│ĀļĀżĒĢ£ ņ░©ļ│äĒÖöļÉ£ ņĀæĻĘ╝ņØ┤ ļÅäņøĆņØ┤ ļÉĀ ņłś ņ׳ļŗż (Fig. 3). PorņØĆ ņłśņ¦üĒśĢ ņä▒ņן Ēī©Ēä┤ņ£╝ļĪ£ ņĀÉļ¦ēĒĢś ņ╣©ļ▓ö ņŚ¼ļČĆņŚÉ ļīĆĒĢ£ ņŗĀņżæĒĢ£ ĒīÉļŗ©ņØ┤, sigņØś Ļ▓ĮņÜ░ļŖö ņłśĒÅēņĀü ņä▒ņן Ēī©Ēä┤ņ£╝ļĪ£ ļ│æļ│Ć Ļ▓ĮĻ│äņŚÉ ļīĆĒĢ£ ņŗĀņżæĒĢ£ ĒīÉļŗ©ņØ┤ ĒĢäņÜöĒĢśļŗż. ļ»ĖļČäĒÖöĒśĢ ņĪ░ĻĖ░ņ£äņĢöņŚÉņä£ ņóģņ¢æ Ļ▓ĮĻ│äņØś ņĀĢĒÖĢĒĢ£ ņśłņĖĪņØä ņ£äĒĢ┤ ņāēņåī ļé┤ņŗ£Ļ▓Į ļ░Å ĒśæļīĆņŚŁ ĒÖĢļīĆļé┤ņŗ£Ļ▓Į(narrow-band imaging with magnifying endoscopy, NBI-ME) ņé¼ņÜ®ņØĆ ļČäĒÖöĒśĢ ņĪ░ĻĖ░ņ£äņĢöļ│┤ļŗż ļÅäņøĆņØ┤ ļÉśņ¦Ć ņĢŖļŗżĻ│Ā ņĢīļĀżņĀĖ ņÖöļŗż[40-42]. sigļŖö ņóģņóģ Ēæ£ņ×¼ņä▒ ņĀÉļ¦ē ļ│ĆĒÖö ņŚåņØ┤ ņāüĒö╝ĒĢś ĒÖĢņé░ Ēī©Ēä┤ņØä ļ│┤ņØ┤ĻĖ░ ļĢīļ¼ĖņØ┤ļŗż. ĻĘĖļ¤¼ļéś ņØ┤Ēøä NBI-MEĻ░Ć ļ│æļ│Ć Ļ▓ĮĻ│ä ĒīÉļŗ©ņŚÉ ļÅäņøĆņØ┤ ļÉ©ņØ┤ ļ│┤Ļ│ĀļÉśņŚłļŖöļŹ░, ņØ┤ļōż ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņĢöņäĖĒż ņ╣©ņ£żņŚÉ ļö░ļźĖ ņĀÉļ¦ēņĖĄņØś ļ│ĆĒÖöļź╝ ļ░öĒāĢņ£╝ļĪ£ NBI-MEņØś ņåīĻ▓¼ņØä extended intervening component pattern(ņĢöņäĖĒżĻ░Ć ņ”ØņŗØ ņśüņŚŁņŚÉ ĻĄŁĒĢ£); wavy microvessel pattern(ņĢöņäĖĒżĻ░Ć Ēæ£ļ®┤ņĖĄņŚÉņä£ ņ”ØņŗØ ņśüņŚŁņ£╝ļĪ£ ĒÖĢņן), corkscrew pattern(ņĢöņäĖĒżĻ░Ć ņĀäņ▓┤ ņĀÉļ¦ēņ£╝ļĪ£ ĒÖĢņן)ņØś 3Ļ░Ćņ¦Ć Ēī©Ēä┤ņ£╝ļĪ£ ļČäļźśĒĢśņśĆļŗż[43-45]. Corkscrew patternņØĆ ļ»ĖļČäĒÖöĒśĢ ņĪ░ĻĖ░ņ£äņĢöņØś NBI-MEņØś ņל ņĢīļĀżņ¦ä ĒśĢĒā£ņØ┤ļéś, ņØ┤ļŖö ņóģņ¢æ ņäĖĒżĻ░Ć ņĀÉļ¦ē ņĀäņ▓┤ļź╝ ņ░©ņ¦ĆĒĢĀ ļĢī Ļ┤Ćņ░░ļÉĀ ņłś ņ׳ļŗż. ņ”ē, ĻĘĖļÅÖņĢł ļŗżļźĖ ļæÉ Ļ░Ćņ¦Ć Ēī©Ēä┤ņØä NBI-MEĻ░Ć ļåōņ│żņØä ņłś ņ׳ņ£╝ļ®░, ņØ┤Ļ▓āņØ┤ ņ¦ĆĻĖłĻ╣īņ¦Ć NBI-MEņØś ņŚŁĒĢĀņØ┤ ļ»ĖļČäĒÖöĒśĢ ņĪ░ĻĖ░ņ£äņĢöņŚÉņä£ ņĀ£ĒĢ£ņĀüņØ┤ņŚłļŹś ņØ┤ņ£ĀņØ┤ļŗż. NBI-MEļŖö sigņŚÉņä£ ņóģņ¢æ ņäĖĒżĻ░Ć ņ░©ņ¦ĆĒĢśļŖö ņ£äņ╣śņŚÉ ļö░ļØ╝ ņØ┤ļ¤¼ĒĢ£ ņäĖ Ļ░Ćņ¦Ć ņ£ĀĒśĢņØä ĻĖ░ļ░śņ£╝ļĪ£ ņóģņ¢æ Ļ▓ĮĻ│äļź╝ ņĀĢĒÖĢĒĢśĻ▓ī ņśłņĖĪĒĢśļŖö ļŹ░ ļÅäņøĆņØ┤ ļÉĀ ņłś ņ׳ļŗż. ņĢäņ¦üĻ╣īņ¦Ć ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ņłĀņŚÉ ņ׳ņ¢┤ņä£ safety marginņŚÉ ļīĆĒĢ£ ņĀĢņØśĻ░Ć ņŚåļŖöļŹ░, ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ ļé┤ņŗ£Ļ▓Į ņÖäņĀä ņĀłņĀ£ ņØ┤Ēøä ņĀłņĀ£ ļ│ĆņŚ░ņŚÉ ņ×öņŚ¼ ņĢöņäĖĒżĻ░Ć ļé©ņĢäņ׳ļŖö Ļ▓ĮņÜ░ļź╝ ļČäņäØĒĢśņśĆņØä ļĢī sig, porņØś ļ»ĖļČäĒÖöĒśĢ ņĪ░ĻĖ░ņ£äņĢöņØś Ļ▓ĮņÜ░Ļ░Ć ņ£äĒŚśņØĖņ×É ņżæ ĒĢśļéśņśĆĻ│Ā, 3 mm ļ»Ėļ¦īņØś safety marginņØ┤ ņ£äĒŚśņØĖņ×É ņżæ ĒĢśļéśņśĆļŗż[46]. ļö░ļØ╝ņä£ ļ»ĖļČäĒÖöĒśĢ ņĪ░ĻĖ░ņ£äņĢöņØś Ļ▓ĮņÜ░ ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ ņØ┤Ēøä ņĀłņĀ£ļ®┤ņŚÉ ņĢöņäĖĒżĻ░Ć ņŚåļŹöļØ╝ļÅä 3 mm ļ»Ėļ¦īņØś safety marginņØĖ Ļ▓ĮņÜ░ņŚÉļŖö ņĀłņĀ£ļ®┤ņŚÉ ņ×öņŚ¼ ņĢöņäĖĒż Ļ░ĆļŖźņä▒ņØä Ļ│ĀļĀżĒĢśņŚ¼ ļ®┤ļ░ĆĒĢ£ ņČöņĀü Ļ┤Ćņ░░ņØ┤ ĒĢäņÜöĒĢĀ ņłś ņ׳ļŗż[46]. ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ ņØ┤Ēøä Ēśäņ×¼ņØś ņÖäņĀä ņĀłņĀ£ ĻĖ░ņżĆņØä ļ▓Śņ¢┤ļéśļ®┤ ņØ╝ļ│ĖņØś Ļ░ĆņØ┤ļō£ļØ╝ņØĖņŚÉņä£ļŖö eCURA ņŗ£ņŖżĒģ£ņŚÉ ņżĆĒĢśņŚ¼ ņČöĻ░Ć ņłśņłĀņØä ĻČīĒĢśĻ│Ā ņ׳ļŗż[32]. ĒĢśņ¦Ćļ¦ī ĻĄŁļé┤ ņŚ░ĻĄ¼ņŚÉ ņØśĒĢśļ®┤ ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ņłĀ ņØ┤Ēøä ņłśĒÅēņĀłņĀ£ņŚ░ ņ╣©ļ▓öļ¦ī ņ¢æņä▒ņØĖ ļČłņÖäņĀä ņĀłņĀ£ņØś Ļ▓ĮņÜ░ļŖö ņłśņłĀņĀü ņĀłņĀ£ Ēøä ļ”╝ĒöäņĀł ņĀäņØ┤Ļ░Ć Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśĻ│Ā[47], ļé┤ņŗ£Ļ▓ĮņĀü ņČöĻ░Ć ņ╣śļŻīļ¦īņ£╝ļĪ£ļÅä ņāØņĪ┤ņ£©ņØ┤ ņÜ░ņłśĒĢ©ņØä ļ│┤Ļ│ĀĒĢśĻ│Ā ņ׳ņ¢┤ņä£ ņČöĻ░Ć ņ╣śļŻī ņĀäļץņŚÉ ļīĆĒĢ┤ņä£ļŖö Ē¢źĒøä ņŚ░ĻĄ¼Ļ░Ć ĒĢäņÜöĒĢśļŗż[48].
ņØ╝ļ░śņĀüņ£╝ļĪ£ Ēś╝ĒĢ®ĒśĢ(mixed-type) ņĪ░ĻĖ░ņ£äņĢöņØś ņśłĒøäĻ░Ć ļČłļ¤ēĒĢśļ®░ ņØ┤ ņżæ ļ»ĖļČäĒÖöĒśĢ ņÜ░ņäĖ Ēś╝ĒĢ®ĒśĢņØś Ļ▓ĮņÜ░ ļŹö ļČłļ¤ēĒĢ£ Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│Ā ļÉśļéś ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ ņĀüņÜ® ļō▒ ņ░©ļ│äņĀü ņ╣śļŻīņĀäļץņØ┤ ĒĢäņÜöĒĢ£ņ¦ĆņŚÉ ļīĆĒĢ┤ ņä£ļŖö ņČöĒøä ņŚ░ĻĄ¼Ļ░Ć ļŹö ĒĢäņÜöĒĢśļŗż[39].
ņ¦äĒ¢ēņä▒ ļ»Ėļ¦īĒśĢ ņ£äņĢöņŚÉņä£ ņłśņłĀņĀü ņ╣śļŻī ļ░Å ņĀäņŗĀĒĢŁņĢöņÜöļ▓ĢņØĆ ņĢäņ¦üĻ╣īņ¦Ć ļ»Ėļ¦īĒśĢ ņ£äņĢöņŚÉņä£ņØś ņ░©ļ│äņĀü ņĀäļץņØ┤ ņĀ£ņŗ£ļÉśĻ│Ā ņ׳ņ¦ĆļŖö ņĢŖļŗż[33]. ņĀäņŗĀĒĢŁņĢöņÜöļ▓ĢņØś Ļ▓ĮņÜ░ HER2 ļ░£ĒśäņŚÉ ļö░ļźĖ ņ╣śļŻī ņäĀĒāØņØ┤ 1ņ░© ņĀäļץņØĖļŹ░[33], ļ»Ėļ¦īĒśĢ ņ£äņĢöņØś Ļ▓ĮņÜ░ ņןĒśĢ ņ£äņĢöņŚÉ ļ╣äĒĢ┤ HER2 ļ░£Ēśäņ£©ņØ┤ ļé«ĻĖ░ ļĢīļ¼ĖņŚÉ ļ»Ėļ¦īĒśĢ ņ£äņĢö ņ╣śļŻīļź╝ ņ£äĒĢ£ ņ╣śļŻī Ēæ£ņĀü ļ░£ĻĄ┤ ļ░Å Ļ░£ļ░£ņØ┤ ĒĢäņÜöĒĢśļŗż.
Ļ▓░ļĪĀ
ļ»Ėļ¦īĒśĢ ņ£äņĢöņØĆ ņןĒśĢ ņ£äņĢöĻ│╝ļŖö ļŗżļźĖ ņĢöĒÖö Ļ│╝ņĀĢ ļ░Å ņāØļ¼╝ĒĢÖņĀü Ē¢ēĒā£ļź╝ ļ│┤ņØĖļŗż. ņ¦äļŗ© ļ░Å ņ╣śļŻīņŚÉ ņ׳ņ¢┤ņä£ ņØ┤ļź╝ Ļ│ĀļĀżĒĢ£ ņĀæĻĘ╝ņØ┤ ņżæņÜöĒĢĀ ņłś ņ׳ņ£╝ļéś ņĢäņ¦üĻ╣īņ¦Ć ļ│æĒā£ņāØļ”¼ņŚÉ ņ׳ņ¢┤ņä£ ņל ĻĘ£ļ¬ģļÉśņ¦Ć ņĢŖņĢśļŗż. ļ»Ėļ¦īĒśĢ ņ£äņĢöņŚÉ ļīĆĒĢ£ ļ│æĒā£ ņāØļ”¼ ĻĘ£ļ¬ģ ļ░Å ņØ┤ļź╝ ĒåĄĒĢ£ ņ╣śļŻīņĀ£ ļ░£ĻĄ┤ ļō▒ņØ┤ ĒĢäņÜöĒĢśĻ▓Āļŗż.