경피 내시경하 위루술 후 발생한 위-대장-피부 누공
Gastro-Colo-Cutaneous Fistula Occurring After Percutaneous Endoscopic Gastrostomy Procedure
Article information

Trans Abstract
An 82-year-old man diagnosed with supraglottic cancer sought a consultation for percutaneous endoscopic gastrostomy (PEG) placement. Preoperative chest radiography (posterior-anterior [PA] view) revealed no abnormalities, and PEG tube placement was performed using the “pull” method. Chest radiography (PA view) performed 3 days postoperatively showed free air that was not observed immediately after PEG tube placement; therefore, the patient was diagnosed with pneumoperitoneum. Abdominal computed tomography confirmed that the PEG tube was appropriately positioned within the stomach; however, the colon was observed between the abdominal wall and stomach, which indicated that the PEG tube had passed through the colon. Review of preoperative chest radiographs (PA views) confirmed that the colon was visualized in the area wherein usually stomach gas should have been observed. The patient was diagnosed with a gastro-colo-cutaneous fistula that occurred postoperatively, following a procedure that was performed without confirmation of anatomical variations. The PEG tube was removed surgically, and we performed percutaneous gastrostomy.
서 론
경피 내시경하 위루술(percutaneous endoscopic gastrostomy, PEG)은 경구 식이가 불가능하여 장기간 관급식을 유지해야 할 환자들에서 널리 시행되고 있는 시술이다. 가장 흔히 쓰이는 방법은 pull method인데, 이 방법은 내시경을 삽입하여 내시경에서 비춰지는 빛을 이용하거나 외부에서 조력자가 복벽을 눌러서 위벽과 복벽이 가장 가까운 위치를 찾는 단계부터 시작한다. 복벽과 위벽의 가장 가까운 위치를 찾은 후 외부에서 침 천자(needle puncture)를 시행하고, 유도 철사(guidewire)를 위 내로 삽입한 후 이 guidewire를 snare나 alligator를 이용하여 잡은 후 내시경과 함께 회수하여 구강 밖으로 빼낸 후 위루관(PEG tube)을 이 guidewire에 연결한 후 조력자가 복부 쪽에서 guidewire를 잡아당김으로써 위 내에 위루관이 거치된다[1]. PEG와 관련된 흔한 합병증에는 복막염, 흡인성 폐렴, 환부 감염, 위나 장의 손상, 출혈, 관 삽입부의 누출(stoma site leakage) 및 관 이탈(migration) 등이 있다[2]. 위-대장-피부 누공(gastro-colo-cutaneous fistula)은 드문 합병증으로 약 0.5%-3%가량 발생한다고 알려져 있는데, 주로 PEG 시술 중 천자를 시행하는 과정에서 복벽과 위벽 사이에 대장이 끼어 있는 것을 모르고 시술하는 경우에 발생하게 된다[3]. 본 증례에서는 PEG 시술 직후에는 발견되지 않았던 공기배증(pneumoperitoneum)이 시술 3일 후에 시행한 흉부 단순 촬영에서 관찰되어서, 추가로 복부 전산화 단층촬영(computed tomography, CT)을 시행한 후 진단된 위-대장-피부 누공의 증례를 보고하고자 한다.
증 례
80세 남자 환자가 식이 후 목으로 액체가 흐르는 증상으로 내원하였다. 환자는 2015년에 성문 상부암(supraglottic cancer) 을 진단받고 수술 및 방사선 치료를 시행했던 환자로, 2023년 5월에 경부 CT상 성문상부에 재발성 종괴가 진단되어 추가로 방사선 치료를 시행하였다. 이후 식사 후 액체가 목에 흐르는 증상이 발견되었고 경부 CT에서 궤양형 종괴로 인해 식도와 피부 사이에 누공이 발생한 것이 의심되었다(Fig. 1). 이에 대해 PEG를 시행하는 것으로 결정이 되어 혈액종양내과로 입원 후 소화기내과에 의뢰되었다. 시술 전 흉부 X-ray에서는 특이 이상 소견이 없었다(Fig. 2). PEG는 pull method로 진행하였고, puncture 위치는 finger indentation method로 복벽과 위벽이 가장 가까운 위치를 확인 후 시술을 시행하였다. 시술 시 별다른 이상이 없이 진행하였고 시술 후 흉부 및 복부 X-ray에서는 특이 이상이 없었다(Fig. 3). 시술 후 환자의 활력징후는 안정적이었으며, 위루관을 통한 식이도 원활하였고 복통도 없는 상태였다. 환자는 종괴에 의한 누공이 의심되는 상황이어서 흡인성 폐렴의 발병을 우려하여 시술 3일 후 별다른 증상이 없었음에도 흉부 X-ray를 추적하였는데, 여기서 공기배증이 발생한 것을 확인하였다. PEG 시술 후 공기배증이 발생하는 것은 흔한 일이지만, 시술 직후 X-ray에서는 별다른 이상이 없었기 때문에, 시술 중 다른 장기 손상이 발생했을 가능성을 염두에 두고 복부 CT를 시행하였다(Fig. 4). CT상 위루관은 위 내로 잘 거치되어 있으나, 위와 복벽 사이에 대장이 끼어서 위루관이 대장을 관통하여 위 내로 삽입되어 있는 상태를 확인하였다. 환자는 아무런 증상이 없었으나, 별다른 준비 없이 위루관을 제거할 경우 복막염이 발생할 것을 우려하여 수술적으로 제거한 후 경피 위루관(percutaneous gastrostomy tube)을 수술적으로 다시 설치하기로 하였다. 복강경으로 관찰하였을 때, S자 결장이 위의 전벽까지 올라와 있었고 PEG tube가 S자 결장을 관통하여 복벽에 고정되어 있음을 확인할 수 있었다(Fig. 5). 분변이 새거나 복막염을 시사하는 소견은 관찰되지 않아서 PEG tube를 제거 후 S자 결장은 단순 봉합을 시행하였고 수술적으로 gastrostomy를 시행하였다. 수술 후 환자는 별다른 합병증 없이 퇴원하였다.

Neck CT of 82-year-old patients with supraglottic cancer. An ulcerative mass has recurred on the supraglottic area, and there is suspicion of a fistula with the skin. CT, computed tomography.

Preoperative chest X-ray. Colon gas is observed in the upper left abdomen, which is the predominant location for gastric gas.
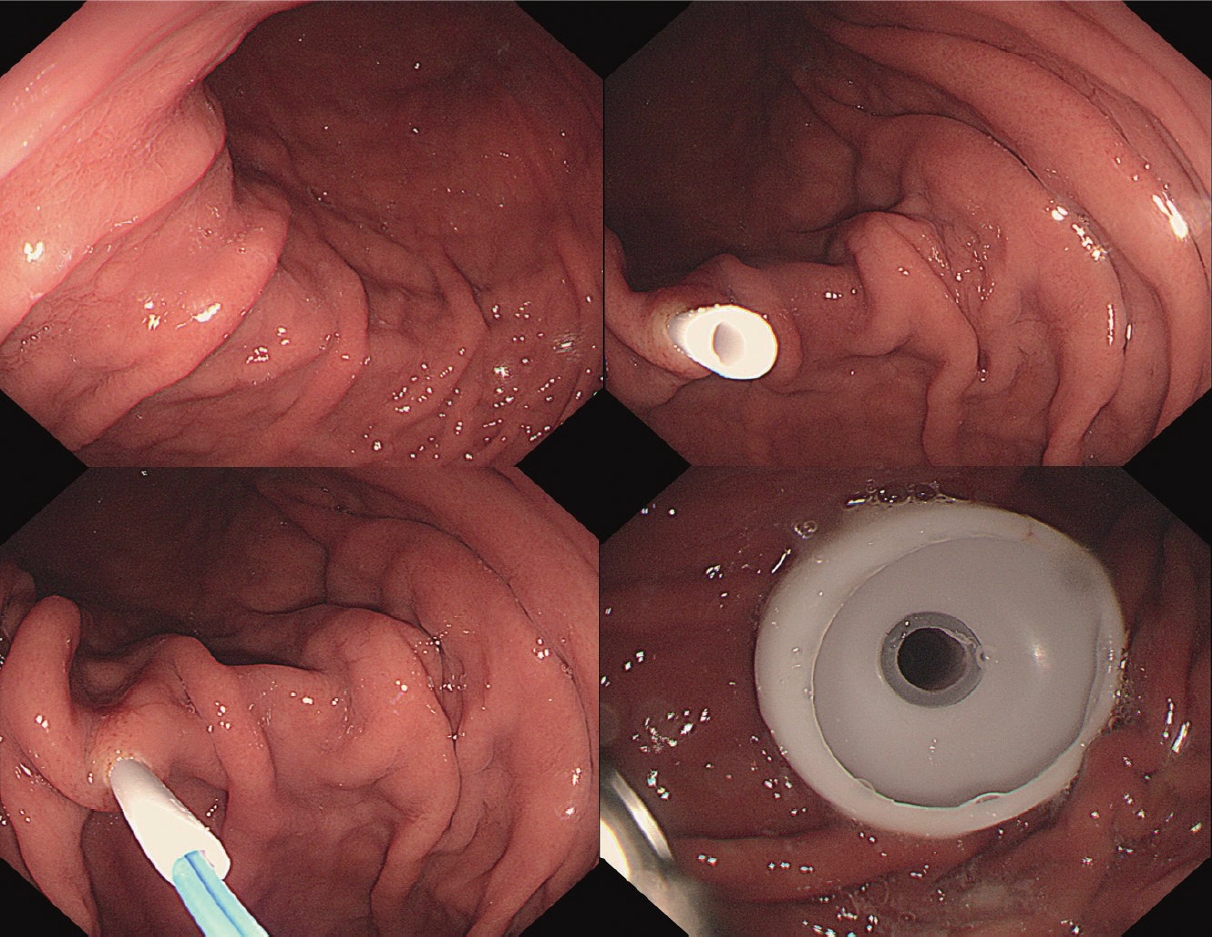
Percutaneous endoscopic gastrostomy was performed using the pull method.
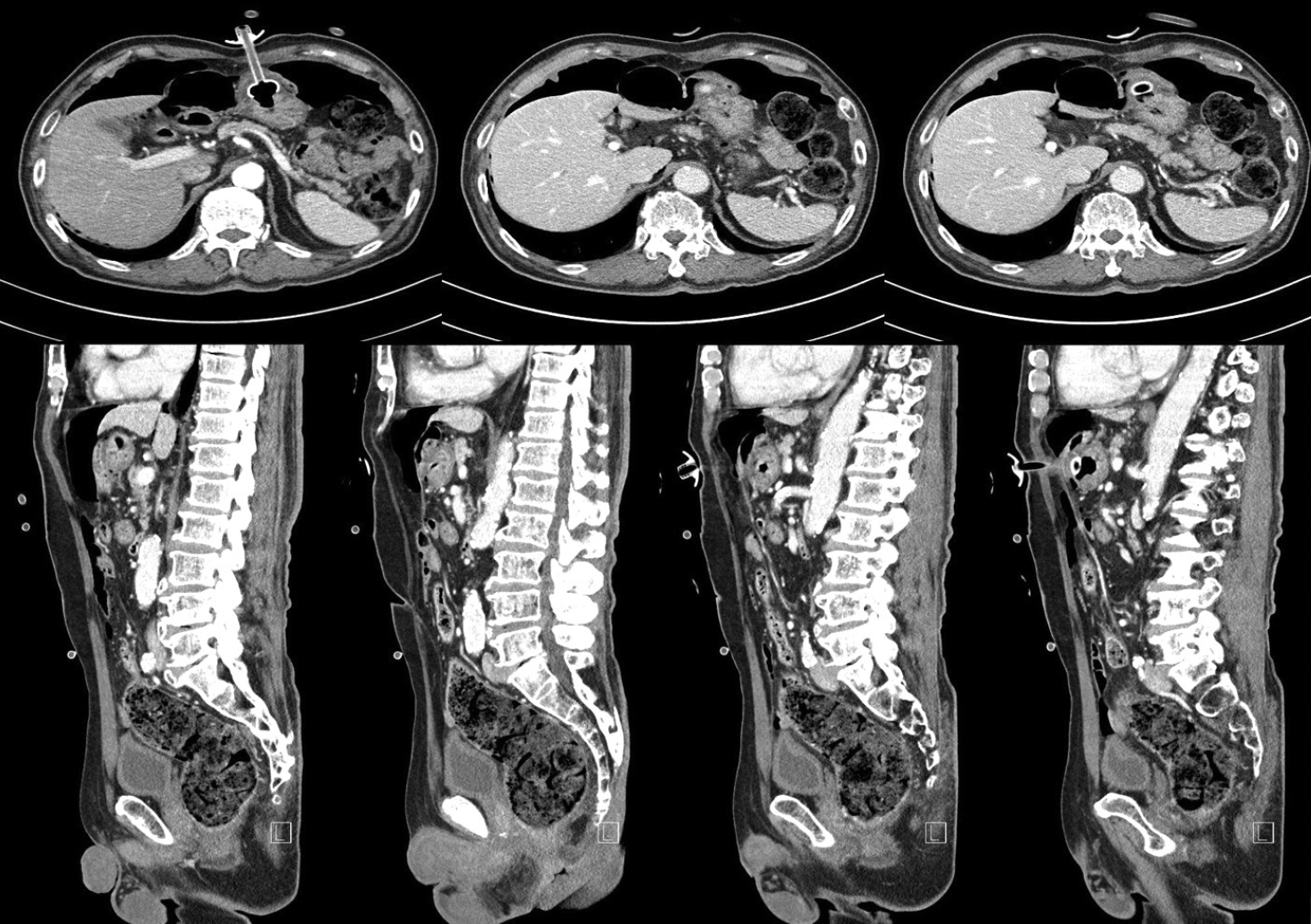
Abdomino-pelvic CT scan. The PEG tube was properly positioned within the stomach, but the colon was situated between the abdominal wall and stomach; hence, the PEG tube passed through the colon. CT, computed tomography; PEG, percutaneous endoscopic gastrostomy.

Laparoscopic image. The sigmoid colon had ascended up to the gastric anterior wall, and the PEG tube was secured to the abdominal wall, passing through the colon. There was no evidence of bowel contents spillage or peritonitis observed. PEG, percutaneous endoscopic gastrostomy.
고 찰
위루관은 보통 한달 이상의 장기간의 관급식이 필요한 경우 내시경적, 수술적, 영상의학적인 방법을 통해 삽입하게 된다. 이중 가장 선호되는 방식은 내시경적으로 pull method를 이용하여 시행하는 방식이다. Pull method는 Ponsky와 Gauderer [4]에 의해 도입된 이후 가장 널리 사용되는 방식으로 내시경을 위 내로 삽입하여 복벽과 위벽이 가장 가까운 위치를 선정하는 과정이 매우 중요한 단계라 할 수 있다. 대부분의 경우 별다른 문제없이 시술을 안전하게 시행할 수 있지만, 복벽과 위벽 사이에 다른 장기가 위치하는 것은 내시경적으로 확인하기 어렵기 때문에 해부학적 변이가 있는 환자에서는 본 증례와 같이 위-대장-피부 누공이 발생할 수 있다.
위-대장 혹은 위-대장-피부 누공은 대략 0.5%-3%에서 발생한다고 알려져 있는데, 대부분의 경우 발생 초기에는 모르고 지내다가 위루관이 이동하여 위에서는 빠져 버리고, 대장 쪽으로 이동하여 위치하게 되면서 환자가 식후에 설사 증상이 발생하면서 알아차리는 경우가 대부분이다[3,5]. 본 증례에서는 특이하게도 별다른 증상이 없었음에도 우연히 흉부 X-ray를 추적하게 되었고 공기배증이 발견되어 원인 평가를 위해 CT를 시행한 후 진단된 증례이다. 위루관에 의한 위-대장-피부 누공이 발생하였음에도 본 증례에서는 위루관이 대장의 정중앙을 관통하였고 위루관에 의해 대장이 복벽쪽으로 잡아당겨져 잘 고정되었기 때문에 복막염이 발생하지 않은 것으로 추정하였다(Fig. 4). 일반적으로는 내시경을 삽입한 후 충분히 송기를 시행하여 위를 팽창시키면 복벽과 위벽을 근접시킬 수 있어서 이와 같은 위-대장-피부 누공은 발생하기 어려우나 해부학적 변이가 있는 경우에는 송기만으로는 해결되지 않는다[6]. 본 증례에서도 시술 전 흉부 X-ray를 살펴보면 좌상복부에서 위 내 가스는 보이지 않고 대장이 위치한 것을 확인할 수 있고, 이러한 해부학적 변이를 간과하고 시술을 진행하였기 때문에 이와 같은 합병증이 발생한 것으로 추정된다(Fig. 2). 이와 같은 합병증을 피하는 또 다른 방법은 내시경의 투과조명(transillumination)을 활용하는 것인데, 이는 내시경에서 강한 빛을 조사하여 복벽에 빛이 비춰지게 하는 방법으로, 이를 통해 복벽과 위벽이 가장 가까운 정확한 위치를 파악하는 데 도움을 얻을 수 있다. 빛이 복벽에서 잘 보이지 않는 경우 다른 장기가 위와 복벽 사이에 위치할 가능성이 있기 때문에 시술하지 않는 것을 고려해야 한다[6]. 본 증례에서는 투과조명을 사용하지 않고 시술을 한 것이 합병증 발생에 영향을 주었을 것으로 판단하였다. PEG 삽입은 크게 pull method와 push method의 두 가지 방법이 알려져 있는데, 본 증례에서는 p ull method를 사용하였다. 두 가지 방법을 비교한 여러 연구에서 colon injury를 포함한 주요 합병증의 발생빈도에서 두 가지 방법이 차이를 보이지 않아서 삽입 방법은 위-대장-피부 누공의 발생에는 기여하지 않았을 것으로 사료된다[7-9]. 본 증례에서와 같이 복벽과 위벽이 떨어져 있을 것으로 추정되는 환자들은 시술 전 CT를 시행하여 해부학적 구조를 반드시 확인하고, 내시경 시술이 어려울 것으로 판단되면 처음부터 수술적으로 위루관을 삽입하는 것을 고려해야 할 것이다.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Conflicts of Interest
Hee Seok Moon, a contributing editor of the Korean Journal of Helicobacter and Upper Gastrointestinal Research, was not involved in the editorial evaluation or decision to publish this article. All remaining authors have declared no conflicts of interest.
Funding Statement
None
Authors’ Contribution
Conceptualization: Sun Hyung Kang. Investigation: Juyung Joung, Jeeyeon Baek. Supervision: Hee Seok Moon, Jae Kyu Sung. Writing—original draft: Juyung Joung. Writing—review & editing: Sun Hyung Kang, Hwan Jung Yun. Approval of final manuscript: all authors.
Ethics Statement
본 증례보고는 환자에게 다른 환자의 진단과 치료를 포함한 의학발전을 위하여 유용하게 사용하려는 학술적 목적으로 본인의 임상정보를 책임저자를 통해 학회지에 양도하는 것에 동의받은 후 작성하였다.
Acknowledgements
None