ņä£ ļĪĀ
ņŗØļÅäņĢöņØĆ ņ¦äļŗ©Ļ│╝ ņ╣śļŻī ļ░®ļ▓ĢņØś ļ░£ņĀäņŚÉļÅä ļČłĻĄ¼ĒĢśĻ│Ā ņśłĒøäĻ░Ć ļ¦żņÜ░ ļČłļ¤ēĒĢ£ ņ£äņןĻ┤Ć ņĢö ņżæņØś ĒĢśļéśņØ┤ļŗż. ņØ┤ļŖö ņŗØļÅäņĢöņØ┤ ņØ┤ļ»Ė ņ¦äĒ¢ēļÉ£ ņāüĒā£ņŚÉņä£ ļ░£Ļ▓¼ļÉśļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦ÄĻ│Ā ļ”╝ĒöäņĀł ņĀäņØ┤Ļ░Ć ĒØöĒĢśĻĖ░ ļĢīļ¼ĖņØ┤ļŗż[1]. ņĀłņĀ£Ļ░ĆļŖźĒĢ£ ņŗØļÅäņĢöņØś Ēæ£ņżĆ ņ╣śļŻīļŖö ņŗØļÅä ņĀłņĀ£ņłĀņØ┤ņ¦Ćļ¦ī ņłśņłĀņŚÉ ļö░ļź┤ļŖö ņØ┤ĒÖśņ£©Ļ│╝ ņé¼ļ¦ØļźĀņØ┤ ļåÆĻ│Ā ņłśņłĀ Ēøä ņéČņØś ņ¦łņØä ĒÜīļ│ĄĒĢśĻĖ░Ļ╣īņ¦Ć ĻĖ┤ ņŗ£Ļ░äņØ┤ ĒĢäņÜöĒĢśļŗżļŖö ņĀ£ĒĢ£ņĀÉņØ┤ ņ׳ļŗż[2,3]. ļ”╝ĒöäņĀł ņĀäņØ┤ Ļ░ĆļŖźņä▒ņØ┤ ņŚåļŖö ņØ╝ļČĆ Ēæ£ņ×¼ņä▒ ņŗØļÅäņĢö(superficial esophageal cancer)ņŚÉ ļīĆĒĢ£ ĻĘ╝ņ╣śņĀü ņĀłņĀ£ ļ¬®ņĀüņ£╝ļĪ£ ļé┤ņŗ£Ļ▓Į ņ╣śļŻīĻ░Ć ņŗ£Ē¢ēļÉśĻ│Ā ņ׳ņ£╝ļ®░, ņŚäĻ▓®ĒĢ£ ņĀüņÜ® ĻĖ░ņżĆņŚÉ ļö░ļź┤ļ®┤ ņ╣śļŻī Ēøä ņāØņĪ┤ņ£©ņØ┤ ņłśņłĀĻ│╝ ļīĆļō▒ĒĢ£ Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│ĀļÉśņŚłļŗż[4]. ņä£ĻĄ¼ņŚÉņä£ļŖö ņŗØļÅä ņāśņĢöņóģ(adenocarcinoma)ņØ┤ ĻĖēĻ▓®Ē׳ ņ”ØĻ░ĆĒĢśĻ│Ā ņ׳ņ£╝ļéś ņÜ░ļ”¼ļéśļØ╝ņŚÉņä£ ļ░£ņāØĒĢśļŖö ņŗØļÅäņĢöņØĆ ļīĆļČĆļČäņØ┤ ĒÄĖĒÅēņäĖĒżņĢöņóģ(squamous cell carcinoma)ņ£╝ļĪ£[5], ļ│Ė ņøÉĻ│ĀņŚÉņä£ļŖö ĒÄĖĒÅēņäĖĒżņĢöņóģņØś ļé┤ņŗ£Ļ▓Į ņ╣śļŻīņŚÉ ļīĆĒĢśņŚ¼ ĻĖ░ņłĀĒĢśĻ│Āņ×É ĒĢ£ļŗż.
ļ│Ė ļĪĀ
1. ļé┤ņŗ£Ļ▓Į ņ╣śļŻīņØś ņĀüņØæņ”Ø
Ēæ£ņ×¼ņä▒ ņŗØļÅäņĢöņØĆ ļ”╝ĒöäņĀł ņĀäņØ┤ņŚÉ Ļ┤ĆĻ│ä ņŚåņØ┤ ņĀÉļ¦ēņĖĄĻ│╝ ņĀÉļ¦ēĒĢśņĖĄņŚÉ ĻĄŁĒĢ£ļÉ£ ņŗØļÅäņĢöņ£╝ļĪ£ ņĀĢņØśĒĢśļ®░, ĻĘĖņżæ ļ”╝ĒöäņĀł ņĀäņØ┤Ļ░Ć ņŚåņ£╝ļ®┤ņä£ ņĀÉļ¦ēņŚÉ ĻĄŁĒĢ£ļÉ£ ņŗØļÅäņĢöņØä ņĪ░ĻĖ░ ņŗØļÅäņĢö(early esophageal cancer)ņØ┤ļØ╝Ļ│Ā ĒĢ£ļŗż. ļé┤ņŗ£Ļ▓Į ņ╣śļŻīņØś ņØ┤ņāüņĀüņØĖ ļ¬®Ēæ£ļŖö ņØ╝Ļ┤ä ņĀłņĀ£ ļ░Å ĻĘ╝ņ╣śņĀü ņĀłņĀ£ņØ┤ļ»ĆļĪ£ ņĪ░ĻĖ░ ņŗØļÅäņĢöĻ│╝ ļ”╝ĒöäņĀł ņĀäņØ┤ Ļ░ĆļŖźņä▒ņØ┤ ļé«ņØĆ ņØ╝ļČĆ Ēæ£ņ×¼ņä▒ ņŗØļÅäņĢöņØ┤ ļé┤ņŗ£Ļ▓Į ņ╣śļŻīņØś ļīĆņāüņØ┤ ļÉ£ļŗż.
ņ╣śļŻī ņĀä ļé┤ņŗ£Ļ▓Į ņ┤łņØīĒīī, ņ╗┤Ēō©Ēä░ļŗ©ņĖĄņ┤¼ņśü, ņ¢æņĀäņ×É ļ░®ņČ£ ļŗ©ņĖĄņ┤¼ņśü ļō▒ņØś Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśņŚ¼ ļ”╝ĒöäņĀł ļ░Å ņøÉĻ▓® ņĀäņØ┤ ņŚ¼ļČĆļź╝ ĒÖĢņØĖĒĢśĻ│Ā ņ×äņāü ļ│æĻĖ░ļź╝ ņäżņĀĢĒĢśļŖö Ļ│╝ņĀĢņØ┤ ĒĢäņÜöĒĢśļŗż[2]. ņŗØļÅäņĢöņØś ĻĄŁņåīņ╣©ņ£ż Ļ╣ŖņØ┤ļź╝ ņśłņĖĪĒĢśļŖö ļŹ░ņŚÉļŖö ļé┤ņŗ£Ļ▓Įņ£╝ļĪ£ Ļ┤Ćņ░░ļÉ£ ņ£ĪņĢł ĒśĢĒā£Ļ░Ć ņżæņÜöĒĢ£ ņŚŁĒĢĀņØä ĒĢ£ļŗż. ņ£ĪņĢłņĀü Ļ┤Ćņ░░ņŚÉ ļö░ļźĖ 0-IĒśĢ(Ēæ£ļ®┤ņ£ĄĻĖ░ĒśĢ) ļśÉļŖö 0-IIIĒśĢ(Ēæ£ļ®┤ĒĢ©ļ¬░ĒśĢ)ņŚÉņä£ļŖö 0-IIĒśĢ(ĒÅēĒāäĒśĢ)Ļ│╝ ļ╣äĻĄÉĒĢśņŚ¼ ņĀÉļ¦ēĒĢś ņ╣©ņ£żņØ┤ ļŹö ļ¦ÄĻ│Ā, ĒÄĖĒÅēĒĢśņ¦Ć ņĢŖņØĆ ņ£ĪņĢł ĒśĢĒā£(0-IIaĒśĢ ļśÉļŖö 0-IIcĒśĢ) ļśÉĒĢ£ ņĀÉļ¦ēĒĢśņĖĄņ£╝ļĪ£ņØś ņ╣©ņ£żņØä ņŗ£ņé¼ĒĢśļ»ĆļĪ£ ļé┤ņŗ£Ļ▓Į ņ╣śļŻīņØś ļīĆņāüņ£╝ļĪ£ļŖö ņĀüĒĢ®ĒĢśņ¦Ć ņĢŖļŗż[6-8]. Ēæ£ļ®┤ņØ┤ ĻĘĀņØ╝ĒĢśņ¦Ć ņĢŖĻ▒░ļéś Ļ▓░ņĀłņāü ļśÉļŖö Ļ│╝ļ”ĮņāüņØ┤ Ļ┤Ćņ░░ļÉśļŖö Ļ▓ĮņÜ░ņŚÉļÅä ņĀÉļ¦ēĒĢśņĖĄ ņ╣©ņ£ż Ļ░ĆļŖźņä▒ņØ┤ ļåÆņ£╝ļ»ĆļĪ£ ņŻ╝ņØśĒĢ┤ņĢ╝ ĒĢ£ļŗż[9]. ņØ┤ņÖĖņŚÉļÅä ļŻ©Ļ│© ņÜ®ņĢĪņØä ļ╣äļĪ»ĒĢ£ ņāēņåī ļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ļź╝ ĒåĄĒĢśņŚ¼ ļ│æļ│ĆņØś Ēü¼ĻĖ░ņÖĆ ļ▓öņ£äļź╝ ļ│┤ļŗż ļ¬ģĒÖĢĒĢśĻ▓ī ĒīīņĢģĒĢĀ ņłś ņ׳ņ£╝ļ®░, ļé┤ņŗ£Ļ▓Į ņ┤łņØīĒīīņÖĆ ņØ┤ļ»Ėņ¦Ć ņ”ØĻ░Ģ ļé┤ņŗ£Ļ▓Į ĻĖ░ļ▓ĢņØä ĒÖ£ņÜ®ĒĢśņŚ¼ ņČöĻ░ĆņĀüņØĖ ņĀĢļ│┤ļź╝ ņ¢╗ņØä ņłś ņ׳ļŗż[10,11].
ņŗØļÅäņĢöņØś ņ╣śļŻī ņĀäļץņØä ņłśļ”ĮĒĢśļŖö ļŹ░ ņ׳ņ¢┤ Ļ░Ćņן ņżæņÜöĒĢ£ ņÜöņåīļŖö ĻĄŁņåī ļ”╝ĒöäņĀł ņĀäņØ┤ Ļ░ĆļŖźņä▒ņØä ņśłņĖĪĒĢśļŖö Ļ▓āņØ┤ļŗż. ļ”╝ĒöäņĀł ņĀäņØ┤ ņ£äĒŚśĻ│╝ ņŚ░Ļ┤ĆļÉ£ ņØĖņ×ÉļĪ£ļŖö ļ│æļ│ĆņØś Ēü¼ĻĖ░, ņ£ĪņĢł ĒśĢĒā£, ļ”╝ĒöäĻ┤Ć ņ╣©ņ£ż(lymphatic invasion) ļō▒ņØ┤ ņĢīļĀżņĀĖ ņ׳ņ£╝ļ®░, ĒŖ╣Ē׳ ņŗØļÅäņĢöņØś ĻĄŁņåīņ╣©ņ£ż ņĀĢļÅäĻ░Ć ļ”╝ĒöäņĀł ņĀäņØ┤ņÖĆ ļ░ĆņĀæĒĢ£ Ļ┤ĆĻ│äĻ░Ć ņ׳ļŗż[6,7,12-15]. Ēæ£ņ×¼ņä▒ ņŗØļÅäņĢöņ£╝ļĪ£ ņłśņłĀņØä ļ░øņØĆ ĒÖśņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ ĒĢ£ ļČäņäØ Ļ▓░Ļ│╝ ņŗØļÅäņĢöņØ┤ ņāüĒö╝ļé┤(intraepithelial, M1) ļśÉļŖö ņĀÉļ¦ēĻ│Āņ£ĀņĖĄ(lamina propria, M2)ņŚÉ ĻĄŁĒĢ£ļÉ£ Ļ▓ĮņÜ░ 0~5.6%ņŚÉņä£ ļ”╝ĒöäņĀł ņĀäņØ┤Ļ░Ć Ļ┤Ćņ░░ļÉśņŚłņ£╝ļ®░, ņóģņ¢æņØ┤ ņĀÉļ¦ēĻĘ╝ņĖĄ(muscularis mucosa, M3)Ļ╣īņ¦Ć ņ╣©ļ▓öĒĢśĻ▒░ļéś ņĀÉļ¦ēĒĢśņĖĄņ£╝ļĪ£ņØś ņ╣©ņ£żņØ┤ 200 ╬╝m ņØ┤ļé┤ņØĖ Ļ▓ĮņÜ░(submucosa 1, SM1) ļ”╝ĒöäņĀł ņĀäņØ┤ņØś ļ╣łļÅäļŖö Ļ░üĻ░ü 9.0~25.0%, 15.0~53.1%ļĪ£ ņ”ØĻ░ĆĒĢśņśĆļŗż[6,12,16]. ļö░ļØ╝ņä£ ņĀÉļ¦ēņĢö ņżæņŚÉņä£ļÅä ļ”╝ĒöäņĀł ņĀäņØ┤ Ļ░ĆļŖźņä▒ņØ┤ Ļ▒░ņØś ņŚåļŖö ņāüĒö╝ļé┤ ļśÉļŖö ņĀÉļ¦ēĻ│Āņ£ĀņĖĄņŚÉ ĻĄŁĒĢ£ļÉ£ Ļ▓ĮņÜ░ļź╝ ļé┤ņŗ£Ļ▓Į ņ╣śļŻīņØś ņĀłļīĆ ņĀüņØæņ”Øņ£╝ļĪ£ ņĀĢņØśĒĢ£ļŗż.
ņØ╝ļ│ĖĻ│╝ ņ£Āļ¤Į, ļ»ĖĻĄŁ Ļ░ĆņØ┤ļō£ļØ╝ņØĖņŚÉņä£ļŖö ņóģņ¢æņØ┤ M3 ļśÉļŖö SM1Ļ╣īņ¦Ć ņ╣©ņ£żĒĢśņśĆļŹöļØ╝ļÅä ļ»ĖņäĖĒśłĻ┤Ć ļśÉļŖö ļ”╝ĒöäĻ┤ĆņŚÉ ņĢöņäĖĒż ņ╣©ņ£żņØ┤ ņŚåļŗżļ®┤ ļ”╝ĒöäņĀł ņĀäņØ┤ņØś ņ£äĒŚśņØ┤ ļé«ņ£╝ļ»ĆļĪ£ ļé┤ņŗ£Ļ▓Į ņ╣śļŻīņØś ņāüļīĆ ņĀüņØæņ”Ø ļśÉļŖö ĒÖĢļīĆ ņĀüņØæņ”Øņ£╝ļĪ£ Ļ│ĀļĀżĒĢ┤ļ│╝ ņłś ņ׳ļŗżĻ│Ā ĻĖ░ņłĀĒĢśĻ│Ā ņ׳ļŗż[8,17,18]. ĻĘĖļ¤¼ļéś ņ╣©ņ£ż Ļ╣ŖņØ┤Ļ░Ć ņ”ØĻ░ĆĒĢ©ņŚÉ ļö░ļØ╝ ļ”╝ĒöäņĀł ņĀäņØ┤ ņ£äĒŚśņä▒ņØ┤ Ļ░ĆĒīīļź┤Ļ▓ī ņ”ØĻ░ĆĒĢśļ»ĆļĪ£ ņ╣śļŻī ņĀä ĒÅēĻ░Ć Ļ▓░Ļ│╝Ļ░Ć M3 ļśÉļŖö SM1 ņ╣©ņ£żņØä ņŗ£ņé¼ĒĢ£ļŗżļ®┤ ļé┤ņŗ£Ļ▓Į ņ╣śļŻīļ│┤ļŗżļŖö ņłśņłĀņØ┤ ņČöņ▓£ļÉśļ®░, ņłśņłĀņŚÉ ļö░ļźĖ ņ£äĒŚśņØ┤ ļåÆņØĆ ņØ╝ļČĆ ĒÖśņ×ÉņŚÉņä£ ņäĀĒāØņĀüņ£╝ļĪ£ ļé┤ņŗ£Ļ▓Į ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢĀ ņłś ņ׳ļŗż.
ļé┤ņŗ£Ļ▓Į ņ╣śļŻī Ēøä ņĀłņĀ£ ņĪ░ņ¦üņŚÉ ļīĆĒĢ£ ļ│æļ”¼ņĪ░ņ¦üĒĢÖņĀü Ļ▓Ćņé¼ Ļ▓░Ļ│╝ņŚÉ ļö░ļØ╝ ĻĘ╝ņ╣śņĀü ņ╣śļŻīļĪ£ ĒīÉļŗ©ĒĢĀ Ļ▓āņØĖņ¦Ć ņČöĻ░Ć ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢĀ Ļ▓āņØĖņ¦Ćļź╝ Ļ▓░ņĀĢĒĢ£ļŗż. ņŗØļÅäņĢöņØ┤ ņĀÉļ¦ēĻĘ╝ņĖĄņØä ņ╣©ņ£żĒĢśņśĆļŹöļØ╝ļÅä ņØ╝Ļ┤ä ņÖäņĀä ņĀłņĀ£ļÉśņŚłĻ│Ā ļČäĒÖöļÅäĻ░Ć ņóŗņ£╝ļ®┤ņä£ ļ»ĖņäĖĒśłĻ┤Ć ļśÉļŖö ļ”╝ĒöäĻ┤Ć ņ╣©ņ£żņØ┤ ņŚåļŗżļ®┤ ņČöĻ░Ć ņ╣śļŻī ņŚåņØ┤ ņĪ░ņŗ¼ņŖżļ¤ĮĻ▓ī Ļ▓ĮĻ│╝ļź╝ Ļ┤Ćņ░░ĒĢ┤ļ│╝ ņłś ņ׳ļŗż[12,17]. ļ│æļ│ĆņØ┤ ļČłņÖäņĀä ņĀłņĀ£ļÉśņŚłĻ▒░ļéś ņĀÉļ¦ēĒĢśņĖĄ ņ╣©ņ£ż, ļ»ĖņäĖĒśłĻ┤Ć ļśÉļŖö ļ”╝ĒöäĻ┤Ć ņ╣©ņ£żņØ┤ ĒÖĢņØĖļÉ£ Ļ▓ĮņÜ░ņŚÉļŖö ĒĢŁņĢö ļ░®ņé¼ņäĀ ņ╣śļŻī ļśÉļŖö ņłśņłĀĻ│╝ Ļ░ÖņØĆ ņČöĻ░Ć ņ╣śļŻīĻ░Ć ĒĢäņÜöĒĢśļŗż[19]. ĻĘĖļ¤¼ļéś ņØ┤ļ¤¼ĒĢ£ ĻĖ░ņżĆņØä ņØ╝Ļ┤äņĀüņ£╝ļĪ£ ņĀüņÜ®ĒĢśĻĖ░ļ│┤ļŗżļŖö ĒÖśņ×ÉņØś ļÅÖļ░ś ņ¦łĒÖśĻ│╝ ņĀäņŗĀ ņāüĒā£, ņłśņłĀņŚÉ ļö░ļź┤ļŖö ņØ┤ĒÖśņ£©Ļ│╝ ņé¼ļ¦ØļźĀņØä Ļ│ĀļĀżĒĢśņŚ¼ ņ╣śļŻī ļ░®Ē¢źņØä Ļ▓░ņĀĢĒĢśļŖö Ļ▓āņØ┤ ļ░öļ×īņ¦üĒĢśļŗż.
2. ņŗØļÅäņĢöņØś ļé┤ņŗ£Ļ▓Į ņ╣śļŻī
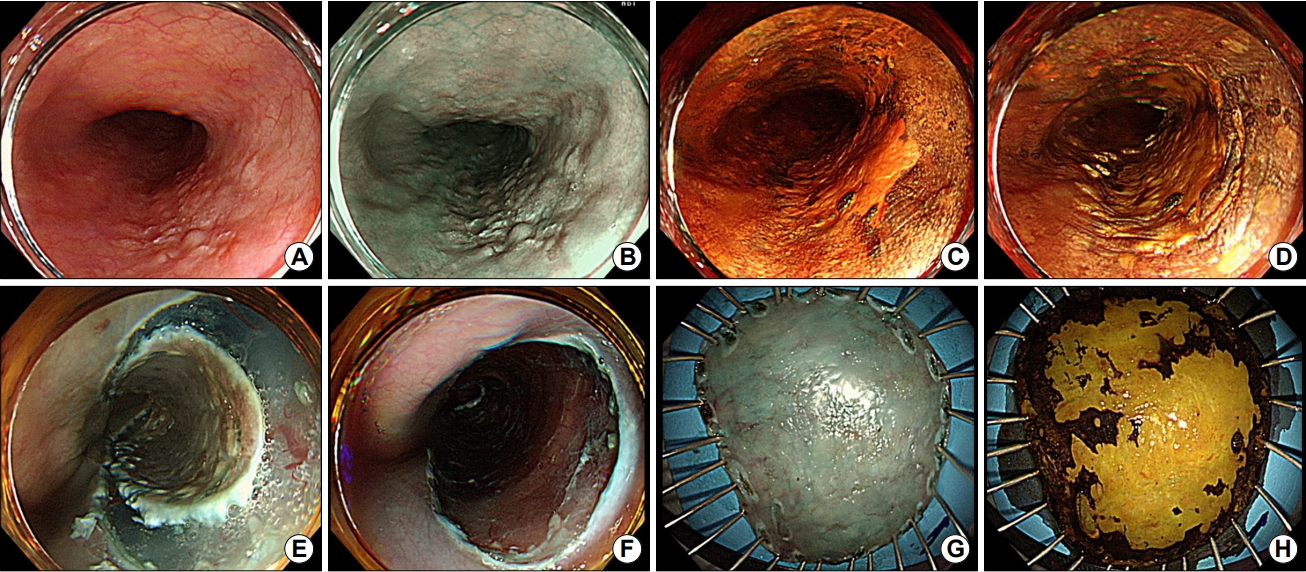
ļé┤ņŗ£Ļ▓Į ņ╣śļŻīņØś ņóģļźśņŚÉļŖö ļé┤ņŗ£Ļ▓Į ņĀÉļ¦ē ņĀłņĀ£ņłĀ(endoscopic mucosal resection), ļé┤ņŗ£Ļ▓Į ņĀÉļ¦ēĒĢś ļ░Ģļ”¼ņłĀ(endoscopic submucosal dissection), ņĢäļź┤Ļ│ż ĒöīļØ╝ņŖżļ¦ł ņåīņ×æņłĀ(argon plasma coagulation), Ļ┤æņŚŁļÅÖ ņ╣śļŻī(photodynamic therapy) ļō▒ņØ┤ ĒżĒĢ©ļÉ£ļŗż. ļ│æļ│ĆņØś ņÖäņĀä ņĀłņĀ£ ļ░Å ņĀłņĀ£ Ēøä ņĪ░ņ¦üņŚÉ ļīĆĒĢ£ ļ│æļ”¼ņĪ░ņ¦üĒĢÖņĀüĻ▓Ćņé¼ļź╝ ņ£äĒĢ┤ņä£ļŖö ņĀÉļ¦ē ņĀłņĀ£ņłĀ ļśÉļŖö ņĀÉļ¦ēĒĢś ļ░Ģļ”¼ņłĀņØ┤ ņČöņ▓£ļÉśļ®░, ĒŖ╣Ē׳ ņĀÉļ¦ēĒĢś ļ░Ģļ”¼ņłĀņØĆ ņĀÉļ¦ē ņĀłņĀ£ņłĀĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ Ēü¼ĻĖ░Ļ░Ć Ēü¼Ļ▒░ļéś ņŗØļÅä ļé┤Ļ░ĢņØä ņÖäņĀäĒ׳ ļæśļ¤¼ņŗĖļŖö ļ│æļ│ĆĻ╣īņ¦ĆļÅä ņØ╝Ļ┤ä ņĀłņĀ£ĒĢĀ ņłś ņ׳ņ¢┤ ņÜ░ņäĀņĀüņ£╝ļĪ£ Ļ│ĀļĀżļÉ£ļŗż(Fig. 1) [20,21].
Ēæ£ņ×¼ņä▒ ņŗØļÅäņĢöņØś ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ņłĀ Ēøä ņ╣śļŻī ņä▒ņĀüņØĆ ļ¦żņÜ░ ņÜ░ņłśĒĢśļŗż. ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ņłĀ Ēøä 402ļ¬ģņØä ĒÅēĻĘĀ 50Ļ░£ņøöĻ░ä ņČöņĀü Ļ┤Ćņ░░ĒĢ£ Ļ▓░Ļ│╝ ņóģņ¢æņØ┤ ņāüĒö╝ļé┤ ļśÉļŖö ņĀÉļ¦ēĻ│Āņ£ĀņĖĄņŚÉ ĻĄŁĒĢ£ļÉ£ Ļ▓ĮņÜ░ 5ļģä ņāØņĪ┤ņ£©ņØĆ 90.5%ņśĆņ£╝ļ®░ ņĀÉļ¦ēĻĘ╝ņĖĄ ļśÉļŖö ņĀÉļ¦ēĒĢś ņ╣©ņ£żņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ Ļ░üĻ░ü 71.1%, 70.8%ļĪ£ ļé«ņØĆ ņāØņĪ┤ņ£©ņØä ļ│┤ņśĆļŗż[22]. ņāØņĪ┤ņ£©Ļ│╝ ņĀäņØ┤ ņ£äĒŚśņØĆ ņóģņ¢æņØś ņ╣©ņ£ż Ļ╣ŖņØ┤ņÖĆ ļ░ĆņĀæĒĢ£ ņŚ░Ļ┤ĆņØ┤ ņ׳ņŚłņ£╝ļ®░, ĒŖ╣Ē׳ ņĀÉļ¦ēņĢöņØ┤ļØ╝ ĒĢśļŹöļØ╝ļÅä ļ»ĖņäĖĒśłĻ┤Ć ļśÉļŖö ļ”╝ĒöäĻ┤Ć ņ╣©ņ£żņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ ņĀäņØ┤ ņ£äĒŚśņØ┤ ņ£ĀņØśĒĢśĻ▓ī ļåÆņĢśļŗż. ļŗżļźĖ ņŚ░ĻĄ¼ņŚÉņä£ ļČäņäØĒĢ£ Ēæ£ņ×¼ņä▒ ņŗØļÅäņĢö 373ņśłņŚÉ ļīĆĒĢ£ ņĀÉļ¦ēĒĢś ļ░Ģļ”¼ņłĀ Ļ▓░Ļ│╝ļŖö ņØ╝Ļ┤ä ņĀłņĀ£, ņÖäņĀä ņĀłņĀ£ņ£©ņØ┤ Ļ░üĻ░ü 96.7%, 84.5%ņśĆņ£╝ļ®░ ĻĘ╝ņ╣śņĀü ņĀłņĀ£ Ēøä 5ļģä ļ¼┤ņ¦łļ│æ ņāØņĪ┤ņ£©(disease-free survival)ņØĆ 84.8%ņśĆļŗż[23].
ĻĄŁļé┤ ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ņŚÉņä£ ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ņłĀ Ēøä ņØ╝Ļ┤ä ņĀłņĀ£ņ£©Ļ│╝ ņÖäņĀä ņĀłņĀ£ņ£©ņØĆ Ļ░üĻ░ü 80.3~97.2%, 81.8~91.7%ļĪ£ ļ│┤Ļ│ĀļÉśņŚłņ£╝ļ®░ ņ╣śļŻī Ēøä ņ×¼ļ░£ ļśÉļŖö ņŗØļÅäņĢö ņŚ░Ļ┤Ć ņé¼ļ¦ØņØś ļ╣łļÅäļŖö ļ¦żņÜ░ ļé«ņĢśļŗż[24-29]. ļŗ©ņØ╝ ĻĖ░Ļ┤ĆņŚÉņä£ ņŗ£Ē¢ēļÉ£ ņ┤Ø 261Ļ░£ ļ│æļ│ĆņŚÉ ļīĆĒĢ£ ņĀÉļ¦ēĒĢś ļ░Ģļ”¼ņłĀ Ļ▓░Ļ│╝ļź╝ ļČäņäØĒĢ£ ņĄ£ĻĘ╝ ņŚ░ĻĄ¼ņŚÉņä£ ņØ╝Ļ┤ä ņĀłņĀ£, ņÖäņĀä ņĀłņĀ£ņ£©ņØĆ Ļ░üĻ░ü 93.9%, 89.7%ņśĆņ£╝ļ®░ ņżæņĢÖĻ░Æ 35Ļ░£ņøö Ļ░äņØś ņČöņĀü Ļ┤Ćņ░░ Ļ▓░Ļ│╝ 5ļģä ņ¦łļ│æ ĒŖ╣ņØ┤ ņāØņĪ┤ņ£©(disease-specific survival)ņØĆ 100%ņśĆļŗż[29]. ļé┤ņŗ£Ļ▓Į ņĀÉļ¦ēĒĢś ļ░Ģļ”¼ņłĀĻ│╝ ņłśņłĀ ņä▒ņĀüņØä ļ╣äĻĄÉĒĢ£ ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ļÅä ļ│┤Ļ│ĀļÉśņŚłļŖöļŹ░, ņä▒Ē¢ź ņĀÉņłś ļ¦żņ╣Ł(propensity score matching) ļ░®ļ▓ĢņØä ņé¼ņÜ®ĒĢśņŚ¼ 120ņīŹņØś ĒÖśņ×Éļź╝ ļ╣äĻĄÉĒĢśņśĆņØä ļĢī ņĀÉļ¦ēĒĢś ļ░Ģļ”¼ņłĀņØä ļ░øņØĆ ĒÖśņ×ÉņØś ņĀäņ▓┤ ņāØņĪ┤ņ£©(overall survival)Ļ│╝ ņ¦łļ│æ ĒŖ╣ņØ┤ ņāØņĪ┤ņ£©ņØĆ 93.9%, 91.2%ļĪ£ ņłśņłĀņØä ļ░øņØĆ ĒÖśņ×ÉņØś ņä▒ņĀü(97.4%, 92.8%)Ļ│╝ ļ╣äĻĄÉĒĢĀ ļ¦īĒĢ£ ņłśņżĆņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż[4]. ņ╣śļŻīņÖĆ ņŚ░Ļ┤ĆļÉ£ ĒĢ®ļ│æņ”ØņØĆ ņłśņłĀņØä ļ░øņØĆ ĒÖśņ×ÉĻĄ░ņŚÉņä£ 55.5%, ļé┤ņŗ£Ļ▓Į ņ╣śļŻīļź╝ ļ░øņØĆ ĒÖśņ×ÉĻĄ░ņŚÉņä£ļŖö 18.5%ļĪ£ ņłśņłĀĻĄ░ņŚÉņä£ ņ£ĀņØśĒĢśĻ▓ī ļŹö ļ¦ÄņØ┤ ļ░£ņāØĒĢśņŚ¼, ļé┤ņŗ£Ļ▓Į ņ╣śļŻīļź╝ ĒåĄĒĢśņŚ¼ ņéČņØś ņ¦łņØä ļ│┤ņĪ┤ĒĢśļ®┤ņä£ ņłśņłĀĻ│╝ ļīĆļō▒ĒĢ£ ņĀĢļÅäņØś ņ╣śļŻīņä▒ņĀüņØä ņ¢╗ņØä ņłś ņ׳ņØīņØä ĒÖĢņØĖĒĢśņśĆļŗż(Table 1).
ļé┤ņŗ£Ļ▓Į ņ╣śļŻīņØś ĒĢ®ļ│æņ”ØņŚÉļŖö ņČ£ĒśłĻ│╝ ņ▓£Ļ│Ą, Ēśæņ░®ņØ┤ ĒżĒĢ©ļÉ£ļŗż. ņŗØļÅäļŖö ļé┤Ļ░ĢņØ┤ ņóüĻ│Ā ĻĄ┤Ļ│ĪņØ┤ ņ׳ņ£╝ļ®░ ņŗ¼ņן ļ░ĢļÅÖ ļśÉļŖö ĒśĖĒØĪņŚÉ ņØśĒĢ£ ņśüĒ¢źņØä ļ░øĻĖ░ ļĢīļ¼ĖņŚÉ ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ņłĀņØ┤ ĻĖ░ņłĀņĀüņ£╝ļĪ£ ņ¢┤ļĀĄļŗż. ļśÉĒĢ£ ņŗØļÅä ļ▓ĮņØĆ ņāüļīĆņĀüņ£╝ļĪ£ ņ¢ćņĢä ņ▓£Ļ│ĄņØś ņ£äĒŚśņØ┤ ļåÆņ£╝ļ®░, ņĀüņØĆ ņ¢æņØś ņČ£ĒśłņŚÉ ņØśĒĢ┤ņä£ļÅä ņŗ£ņĢ╝Ļ░Ć ņēĮĻ▓ī ļéśļ╣Āņ¦ĆĻĖ░ ļĢīļ¼ĖņŚÉ ņ¦ĆĒśłņŚÉ ņ¢┤ļĀżņøĆņØä Ļ▓¬ņØä ņłś ņ׳ļŗż. ņØ┤ļ¤¼ĒĢ£ ĒĢ┤ļČĆĒĢÖņĀü ņÜöņØĖ ņØ┤ņÖĖņŚÉļÅä ņŗ£ņłĀņ×ÉņØś Ļ▓ĮĒŚśĻ│╝ ņłÖļĀ©ļÅä ļśÉĒĢ£ ĒĢ®ļ│æņ”Ø ļ░£ņāØņŚÉ ņśüĒ¢źņØä ļ»Ėņ╣śļŖö ņØĖņ×É ņżæ ĒĢśļéśļĪ£, ņĢłņĀäĒĢ£ ņ╣śļŻīļź╝ ņ£äĒĢ┤ņä£ļŖö ņłÖļĀ©ļÉ£ ļé┤ņŗ£Ļ▓Į ņØśņé¼Ļ░Ć ņĀäņŗĀ ļ¦łņĘ©ĒĢśņŚÉ ņŗ£ņłĀņØä ņŗ£Ē¢ēĒĢśļŖö Ļ▓āņØ┤ ļ░öļ×īņ¦üĒĢśļŗż[23]. ņŗ£ņłĀĻ│╝ ņŚ░Ļ┤ĆļÉ£ ņČ£ĒśłņØĆ 0~5.6%, ņ▓£Ļ│ĄņØĆ 4~9.3%ņŚÉņä£ ļ│┤Ļ│ĀļÉśņŚłņ£╝ļ®░, ļīĆļČĆļČä ļé┤ņŗ£Ļ▓Į ņ¦ĆĒśłņłĀ ļśÉļŖö ļ┤ēĒĢ®ņłĀņØä ĒåĄĒĢśņŚ¼ ņä▒Ļ│ĄņĀüņ£╝ļĪ£ ņ╣śļŻīĒĢĀ ņłś ņ׳ņŚłļŗż[4,23,24,26-30].
ņŗØļÅäņĢöņØś ļé┤ņŗ£Ļ▓Į ņ╣śļŻīņŚÉņä£ ļ░śļō£ņŗ£ Ļ│ĀļĀżļÉśņ¢┤ņĢ╝ ĒĢĀ ņĀÉņØĆ ņ╣śļŻī Ēøä ļ░£ņāØĒĢĀ ņłś ņ׳ļŖö Ēśæņ░®ņŚÉ ļīĆĒĢ£ ņśłļ░®Ļ│╝ ļīĆņ▓śņØ┤ļŗż. ļé┤ņŗ£Ļ▓Į ņ╣śļŻī Ēøä Ēśæņ░®ņØĆ 5.4~13.9%ņŚÉņä£ ļ░£ņāØĒĢśļ®░, ĒŖ╣Ē׳ ņĀłņĀ£ Ēøä ņĀÉļ¦ē Ļ▓░ņåÉņØ┤ ņøÉņŻ╝ņØś 75% ņØ┤ņāüņØä ņ░©ņ¦ĆĒĢśļŖö Ļ▓ĮņÜ░ Ēśæņ░®ņØś ņ£äĒŚśņØ┤ ļ¦żņÜ░ ļåÆņ£╝ļ»ĆļĪ£ Ēśæņ░® ņśłļ░®ņØä ņ£äĒĢ£ ņĪ░ņ╣śĻ░Ć ĒĢäņÜöĒĢśļŗż[4,23,24,26-29,31,32]. Ēśæņ░® ļ░£ņāØ ņśłļ░® ļ░Å ņ╣śļŻī ļ░®ļ▓Ģņ£╝ļĪ£ ĒÆŹņäĀĒÖĢņןņłĀņØä ņŗ£Ē¢ēĒĢĀ ņłś ņ׳ņ£╝ļéś ļīĆĻ░£ ļ░śļ│ĄņĀüņØĖ ņŗ£ņłĀņØ┤ ĒĢäņÜöĒĢśļŗż[33-35]. ņØ╝ņŗ£ņĀüņ£╝ļĪ£ ņŖżĒģÉĒŖĖļź╝ ņéĮņ×ģĒĢśņśĆļŗżĻ░Ć ņĀ£Ļ▒░ĒĢśļŖö ļ░®ļ▓ĢļÅä ņé¼ņÜ®ĒĢ┤ļ│╝ ņłś ņ׳ļŗż[36]. ļé┤ņŗ£Ļ▓Į ņĀłĻ░£ļÅäļź╝ ņé¼ņÜ®ĒĢśņŚ¼ Ēśæņ░® ļČĆļČäņØä ņ¦üņĀæ ņĀłĻ░£ĒĢśļŖö ļ░®ļ▓ĢļÅä ņŗ£ļÅäļÉśņŚłņ£╝ļéś ņČ£ĒśłĻ│╝ ņ▓£Ļ│ĄņŚÉ ļīĆĒĢ£ ņŻ╝ņØśĻ░Ć ĒĢäņÜöĒĢśļ®░ ņןĻĖ░ ņä▒ņĀüņŚÉ ļīĆĒĢ£ ņŚ░ĻĄ¼Ļ░Ć ļŹö ĒĢäņÜöĒĢśļŗż[37,38]. ņŗ£ņłĀ Ēøä Ēśæņ░®ņØ┤ ņśłņāüļÉśļŖö ĒÖśņ×ÉņŚÉņä£ ņŗ£ņłĀ ņ¦üĒøä ņĀÉļ¦ēĒĢśņĖĄņŚÉ ĻĄŁņåī ņŖżĒģīļĪ£ņØ┤ļō£ļź╝ ņŻ╝ņ×ģĒĢśĻ▒░ļéś Ļ▓ĮĻĄ¼ ņŖżĒģīļĪ£ņØ┤ļō£ļź╝ ņé¼ņÜ®ĒĢ©ņ£╝ļĪ£ņŹ© Ēśæņ░® ļ░£ņāØņØä ņżäņØ╝ ņłś ņ׳ļŗż[33,39,40]. ņ┤Ø 12Ļ░£ ņŚ░ĻĄ¼, 513ļ¬ģņØä ĒżĒĢ©ĒĢ£ ļäżĒŖĖņøīĒü¼ ļ®öĒāĆļČäņäØ Ļ▓░Ļ│╝ņŚÉņä£ļÅä ĻĄŁņåī ļśÉļŖö Ļ▓ĮĻĄ¼ ņŖżĒģīļĪ£ņØ┤ļō£ļź╝ ņé¼ņÜ®ĒĢ©ņ£╝ļĪ£ņŹ© ļīĆņĪ░ĻĄ░Ļ│╝ ļ╣äĻĄÉĒĢśņŚ¼ Ēśæņ░® ņ£äĒŚśņØä Ļ░Éņåīņŗ£ĒéżĻ│Ā ĒÆŹņäĀĒÖĢņןņłĀ ņ╣śļŻī Ēܤņłśļź╝ ņżäņØ╝ ņłś ņ׳ņŚłļŗż[41]. ĻĘĖļ¤¼ļéś Ēśæņ░®ņŚÉ ļīĆĒĢ£ ņśłļ░® ļ░Å ņ╣śļŻī ļ░®ļ▓ĢņØĆ ņĢäņ¦üĻ╣īņ¦Ć Ēæ£ņżĆĒÖöļÉśņ¢┤ ņ׳ņ¦Ć ņĢŖņ£╝ļ®░, ņØ┤ļ»Ė ņĢīļĀżņ¦ä ļ░®ļ▓ĢļōżņØś ĒÜ©Ļ│╝ļź╝ ļ╣äĻĄÉĒĢśļŖö ņŚ░ĻĄ¼ļ┐Éļ¦ī ņĢäļŗłļØ╝ ņāłļĪ£ņÜ┤ ļ░®ļ▓ĢņŚÉ ļīĆĒĢ£ ņŗ£ļÅäļōżņØ┤ ņŚ¼ņĀäĒ׳ ĒĢäņÜöĒĢśļŗż.
Ļ▓░ ļĪĀ
ņŗØļÅäņĢöņØś ļé┤ņŗ£Ļ▓Į ņ╣śļŻīļŖö ņĪ░ĻĖ░ ņŗØļÅäņĢö ļ░Å ļ”╝ĒöäņĀł ņĀäņØ┤ Ļ░ĆļŖźņä▒ņØ┤ ļ¦żņÜ░ ļé«ņØĆ Ēæ£ņ×¼ņä▒ ņŗØļÅäņĢöņØś ņØ╝ļČĆļź╝ ļīĆņāüņ£╝ļĪ£ ĒĢ£ļŗż. ļé┤ņŗ£Ļ▓Į ņ╣śļŻīļź╝ ĒåĄĒĢśņŚ¼ ņ╣śļŻī ĻĖ░Ļ░äņØä ļŗ©ņČĢĒĢśĻ│Ā ņéČņØś ņ¦łņØä ļ│┤ņĪ┤ĒĢĀ ņłś ņ׳ņ£╝ļ®░, ņןĻĖ░ ņČöņĀü Ļ▓░Ļ│╝ņŚÉ ņ׳ņ¢┤ņä£ļÅä ņłśņłĀĻ│╝ ļ╣äĻĄÉĒĢĀ ļ¦īĒĢ£ ņ╣śļŻī ņä▒ņĀüļōżņØ┤ ļ│┤Ļ│ĀļÉśņ¢┤ ņłśņłĀņØä ļīĆņŗĀĒĢśļŖö ĻĘ╝ņ╣ś ļ¬®ņĀüņ£╝ļĪ£ ņŗ£Ē¢ēļÉśĻ│Ā ņ׳ļŗż. ņĀÉļ¦ēĒĢśņĖĄ ņ╣©ņ£żņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ ļ”╝ĒöäņĀł ņĀäņØ┤ ņ£äĒŚśņØ┤ ņ”ØĻ░ĆĒĢ£ļŗżļŖö ņĀÉņŚÉ ņ£ĀņØśĒĢśņŚ¼ ņ╣śļŻī ņĀäļץņØä ņłśļ”ĮĒĢśļŖö Ļ▓āņØ┤ ņżæņÜöĒĢśļ®░, ņĀłņĀ£ ņĪ░ņ¦üņŚÉ ļīĆĒĢ£ ļ│æļ”¼ ņĪ░ņ¦üĻ▓Ćņé¼ Ļ▓░Ļ│╝ļź╝ ņĀüņĀłĒĢśĻ▓ī ĒĢ┤ņäØĒĢśĻ│Ā ņČöĻ░Ć ņ╣śļŻī ņŚ¼ļČĆļź╝ Ļ▓░ņĀĢĒĢĀ ņłś ņ׳ņ¢┤ņĢ╝ ĒĢ£ļŗż. ļśÉĒĢ£ ņŗØļÅä ņøÉņŻ╝ņØś 75% ņØ┤ņāüņØä ņĀłņĀ£ĒĢśļŖö Ļ▓ĮņÜ░ ņŗ£ņłĀ Ēøä Ēśæņ░® ļ░£ņāØ Ļ░ĆļŖźņä▒ņØ┤ ļåÆņØīņØä ņŚ╝ļæÉņŚÉ ļæÉĻ│Ā ņśłļ░® ņĪ░ņ╣śļź╝ ņŗ£Ē¢ēĒĢ┤ņĢ╝ ĒĢ£ļŗż.