위마비로 오인된 공장선암
Adenocarcinoma of the Proximal Jejunum Misdiagnosed as Gastroparesis
Article information
 , 조민재, 하소영, 서민지, 문상곤, 오정환
, 조민재, 하소영, 서민지, 문상곤, 오정환
Trans Abstract
The prevalence of small bowel cancer is relatively low. The abdominal pain that patients with small bowel cancer present as a symptom is non-specific and often interpreted as a normal finding on radiographic studies. To prevent delayed diagnosis of small bowel cancer, practitioners must maintain a certain level of suspicion. We report a case of delayed diagnosis of jejunal cancer as it was misdiagnosed as gastroparesis. A 69-year-old woman complained of recurrent nausea and vomiting. At the beginning of her hospitalization, we could not diagnose mechanical obstruction through esophagogastroduodenoscopy and abdominal computed tomography. A gastric emptying study revealed delayed gastric emptying. Although the patients received treatments, including administration of prokinetics and botulinum toxin injection, for gastroparesis, her symptoms aggravated. Subsequently, plain radiography of the abdomen revealed a double-bubble sign. Abdominal computed tomography was performed under the suspicion of small bowel obstruction; however, the diagnosis was not clear. Consequently, exploratory laparoscopy was performed. She underwent surgical management, including small bowel segmental resection and duodenojejunostomy, due to the jejunal mass with involvement of the stomach, pancreatic head, and mesentery of the transverse colon. The postoperative pathological results revealed a moderately differentiated adenocarcinoma of the jejunum.
서 론
소장암은 소화관 악성 종양의 1.1~2.4%를 차지한다. 드문 질환이면서 증상이 뚜렷하지 않은 경우가 많아 진단에 어려움이 있다. 이 증례에서는 기능성 소화불량증, 과민성 대장증후군으로 10년간 소화기내과 외래에서 약물 치료를 하면서 소화 불량, 복통의 호전과 악화를 반복한 환자에서 공장암이 병발하였으나 위내시경, 복부 전산화단층촬영에서 기질적 질환을 진단하지 못하였고, 핵의학 검사에서 위배출 시간이 지연된 것으로 특발성 위마비로 오인하여 진단이 늦어진 증례를 경험하여 보고하는 바이다.
증 례
69세 여자가 1년 전부터 식후 구역, 구토가 시작되었고 최근 4개월 동안에는 증상이 지속되어 입원하였다. 소화 불량, 설사, 복통 등의 증상으로 10년 전부터 소화기내과 진료를 보았고 검사 결과 기질적인 문제가 없어 기능성 소화불량증, 과민성 대장증후군 진단 하에 약물 치료하면서 외래 추적 관찰하였다. 내원 1년 전부터 식후 구역, 복통으로 반복적인 입·퇴원을 6차례 하였고 입원 기간에 복부 전산화단층촬영(1회), 위내시경(2회), 대장내시경(1회)을 시행하였으나 검사 결과 이상은 없었다. 내원 4개월 전부터 식후 구역, 구토, 복통이 지속되어 재입원을 하였다.
과거력에서 고혈압, 갑상샘 저하증, 우울증이 있었으며 음주력과 흡연력은 없었다. 복부 수술력은 자궁 용종으로 전자궁 절제술을 20년 전에 시행하였다. 활력징후는 혈압 100/70 mmHg, 맥박은 분당 90회, 호흡수는 분당 18회, 체온 36.8℃였고 의식은 명료하였다. 계통별 문진에서 식욕이 감소하여 있었고 5개월 동안 체중 감소가 10 kg 정도 있었다. 식후 1시간 이내 구역, 구토가 있었고 구토물의 색깔은 명확하지는 않았다. 위치를 정확하게 명시하지 못하는 간헐적인 복통을 숫자 평가 척도(numeric rating scale) 5점으로 호소하였고 지속 시간은 10분 전후, 횟수는 하루에 5번 이상 있었으며 식후 통증을 호소하는 경향이 있었다. 신체 진찰에서 전반적인 복부 팽만이 있고 장음은 감소되어 있었다. 명치와 좌상부에 경계가 불분명하며 단단한 비정상적인 덩어리가 약 5×5 cm 크기로 만져졌다. 복벽에 힘을 주었을 경우 만져지지 않고 압통이 있었다. 검사실 소견으로 백혈구 6,100/mm3, 혈색소 12.6 g/dL, 혈소판 173,000/mm3, AST/ALT 16/9 IU/L, BUN 4.2 mg/dL, creatinine 0.65 mg/dL, sodium 140 mmol/L, potassium 3.4 mmol/L, CRP <0.01 mg/dL였다. 잠혈 검사는 음성이었다. 갑상선 기능검사는 thyroid-stimulating hormone 1.67 μIU/mL, triiodothyronine 82.7 ng/dL, free thyroxine 1.04 ng/dL였고, 암표지자 carcino-embryonic antigen 3.12 ng/mL로 정상이었다. 단순 복부 X-선 검사에서 특이 소견은 없었고 복부 전산화단층촬영을 시행하였다. 1년 전에 시행한 복부 전산화단층촬영과 비교하여 위와 십이지장 1, 2, 4부가 눈에 띄게 늘어나 있었고 십이지장 3부는 좁아져 있었다. 위장관의 기계적인 폐쇄에 대한 감별을 위하여 위내시경, 저장성 십이지장 조영술(hypotonic duodenography)을 시행하였다. 위내시경에서 담즙 역류가 확인되었으며 십이지장 2부까지 폐쇄 병변은 없었다. 저장성 십이지장 조영술에서 십이지장 3부가 좁아져 있었다. 위장관 운동 촉진제(mosapride 5 mg 경구 하루 3번, metoclopramide 10 mg 정주 하루 3번)를 투여하면서 입원 8일째 증상의 호전을 보여 퇴원하였으나 외래에서 증상 악화를 보여 퇴원한지 15일 만에 재입원하였다. 재입원 4일째 방사선 동위원소를 이용하여 위배출 시간을 측정하였다. 방사선 표지자로 5 mCi의 Tc-99m sulfur colloid를 계란에 섞어 고형식 형태로 섭취하게 한 후 기립 자세로 15분 간격으로 60초씩 120분에 걸쳐 전면, 후면상을 얻었다. 위배출 시간(T1/2)은 237.9분으로 심한 위배출능의 장애를 확인하였다(Fig. 1) 위마비 진단 하에 위장관 운동 촉진제인 mosapraide 5 mg씩 하루 3회 경구로 20일을 투여하였고, metoclopramide hydrochloride 10 mg씩 하루 3회 정맥으로 30일 이상 투여하였으나 증상 호전은 없었다. 유문륜에 보툴리눔 독소 주사를 시행하기 위하여 재입원 13일째에 위 내시경을 시행하였고 위에 많은 양의 담즙을 확인하였다(Fig. 2) 이 소견으로 유문부 이하 부위의 폐쇄 가능성을 고려하였으나 복부 전산화단층촬영을 시행한지 한 달이 되지 않았고, 그 당시 기계적 폐쇄가 확인되지 않았기에 원래 계획하였던 대로 보툼리눔 독소 주사를 시행하였다. 보툴리눔 독소 100 unit을 4 mL의 생리식염수에 희석하고 유문륜 주위 4방향에 각각 1 mL씩 주입하였다. 이후 환자는 일부 증상의 호전을 보여 보툼리눔 독소 주사를 입원 35일째 재시행하였다. 이후 복통과 함께 담즙성 구토의 악화를 보이고 단순 복부 X-선 검사에서 쌍방울 징후(double-bubble sign)를 확인하였다(Fig. 3A) 이 소견을 바탕으로 소장 폐쇄 의심 하에 복부 전산화단층촬영을 진행하였고 십이지장 공장 이음부의 비정상적인 위치와 이행을 확인하였다(Fig. 3B) 진단이 명확하지 않아 재입원 55일째에 진단적 복강경을 시행하였고, 공장 근위부에 2.0×1.5 cm 종괴와 함께 위, 췌장 두부와 횡행결장 장간막에 암 침윤 소견을 확인하여 장 부분 절제술, 샘공장연결술을 시행하였다(Fig. 4A) 병리검사 결과 최종 진단으로 공장선암을 확인하였다(Fig. 4B) TNM staging (T4NxM1)을 확인하고 1년간 보조 항암화학요법으로 5-fluorouracil/leucovorin을 6차례 진행하고 XELOX (capecitabine plus oxaliplatin)를 3차례까지 진행하였으나 암이 진행하면서 전신 상태가 악화되어 항암 치료를 중단하였고 수술 후 1년 5개월째에 사망하였다.
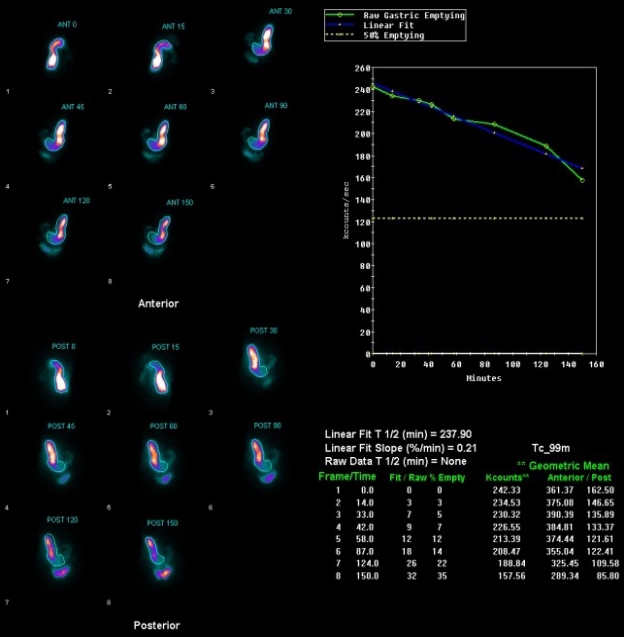
Gastric emptying time. It takes approximately 237 minutes for 50 percent of ingested food to be expelled from the stomach.

(A, B) Endoscopic findings showing excessive bile reflux.
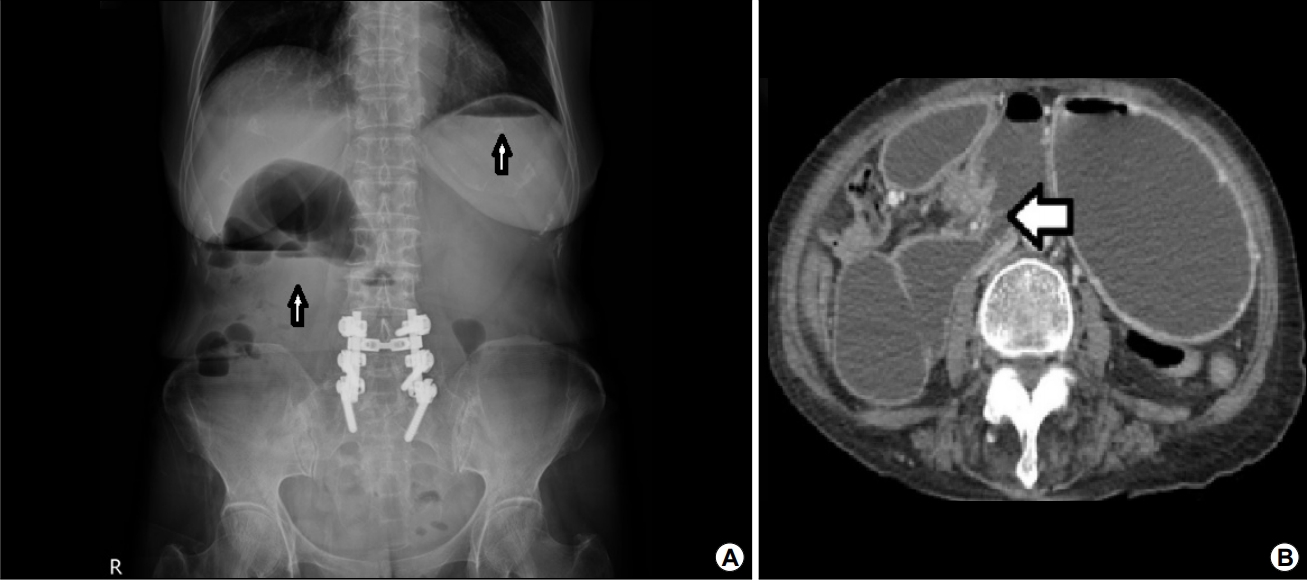
(A) Abdominal radiography and CT images. The upright abdominal radiograph shows a double-bubble sign (white arrows). (B) The contrast-enhanced CT scan shows the abnormal position and abrupt transition of the duodenojejunal junction (white arrow).
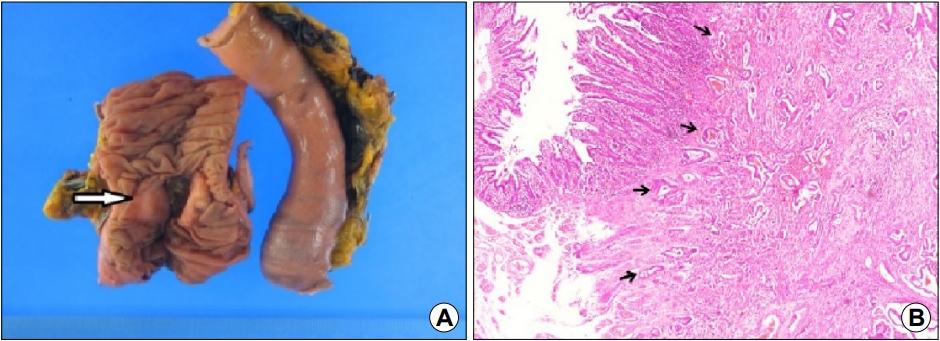
Gross and pathological findings of the surgical specimen. (A) An ulceroinfiltrative mass measuring 2.0×1.5 cm in size is observed in the proximal jejunum (white arrow). (B) The microscopic findings show a typical moderately differentiated adenocarcinoma (H&E, ×40; black arrows).
고 찰
소장은 전체 소화관 길이의 3/4, 면적의 9/10이지만 소장암은 전체 위장관 종양의 3% 이내로 드물다[1]. 소장암은 예후가 좋지 않아서 조기에 진단을 하는 것이 중요하다[2]. 증상이 비특이적이고 진단 방법에도 한계가 있어 진단이 늦춰지는 경우가 많다[3]. 복부 전산화단층촬영의 소장암에 대한 정확도는 50% 정도로 높지 않다[4,5]. 증상이 명확하지 않기 때문에 특히 기능성 소화불량증이나 과민성 장증후군 환자에서 소장암이 병발하였을 때는 진단이 지연될 가능성이 높다[6].
위마비는 기계적 폐색과 같은 기질적인 원인이 없으면서 위마비 증상이 있고 위배출의 지연이 확인된 경우로 정의한다[7]. 구역, 구토, 조기 포만감, 체중 감소 등의 증상이 반복적으로 나타나는 환자에서 위내시경, 복부 초음파, 위장 조영술, 복부 전산화단층촬영 등을 시행하여 기질적인 원인이 없음을 확인하고 위배출 시간 측정을 통하여 위마비를 진단한다. 소장은 여러 검사 방법에서 위음성으로 확인될 가능성이 있다. 이러한 이유로 소장암에 의한 폐색이 원인이 되어 위배출 지연이 있는 경우에 위마비로 오인되어 진단이 지연될 가능성이 있다. 특히 원인을 설명할 수 없는 반복적인 경련성 복통이 있는 경우, 염증성 장질환이나 이전 복부 수술력이 없는데 장 폐쇄가 있는 경우, 성인에서 장중첩증이 동반되는 경우, 위와 대장내시경 검사 외에 일반적인 영상 검사에서 정상으로 확인되는 만성적인 장출혈이 있는 경우 소장 종양을 의심하고 소장을 평가할 수 있는 검사를 진행하는 것이 필요하다. 소장암을 진단하기 위하여 캡슐내시경, 가압소장내시경(push enteroscopy), 고압관장법(enteroclysis) 등을 진행하고 CT/MR 소장조영술, 풍선소장내시경까지 적극적으로 고려하는 것이 필요하다[8,9].
위마비로 오인된 소장암에 대한 증례 보고는 현재까지 국내에는 없으며 국외에 몇 예가 있고 그중 3예를 Table 1에 정리하였다[10-12]. 본 증례는 기능성 소화불량증, 과민성 장증후군으로 10년 정도의 기간 동안 외래에서 치료한 환자라는 점에서 이전에 보고되었던 증례와 차이가 있다. 즉 기능성 소화기 질환 환자에서 비특이적인 복부 증상을 반복적으로 호소할 때 기질적인 문제보다는 기능성 질환이라는 낙인(stigmata)을 찍고 추가적인 평가를 하지 않을 가능성이 높다. 소장암은 증상이 비특이적이고 일반적인 위내시경이나 복부 전산화단층촬영으로 진단하는 데 어려움이 있어서 의심을 해야 진단을 할 수 있다. 본 증례는 복부 전산화단층촬영에서 십이지장 3부의 좁아진 부분에 대하여 가압소장내시경, 풍선소장내시경 등을 이용한 적극적인 평가를 진행하지 않고 특발성 위마비로 진단을 하였고, 외래에서 오랜 기간 동안 치료한 기능성 소화기 질환 환자라는 점에서 기질적인 문제가 새롭게 동반되었을 가능성을 낮게 보고 적극적인 평가를 시행하지 못한 면이 있다[13,14].

Summary of Other Cases with Similar Clinical Features
위마비에 대한 치료는 식이 조절과 위장관 운동 촉진제, 항구토제 등의 약물 치료가 있다[7]. 위장관 운동 촉진제의 경구 투여가 입원 기간이나 재입원율에 영향을 미치지는 못하였으나 위장관운동 촉진제의 정맥 투여는 입원 기간을 줄이는 데 영향이 있다는 보고가 있다[15]. 이외에도 유문부 경련(pylorospasm)이 일부 위마비의 원인으로 인식되면서 보툴리눔 독소를 유문부에 주입하는 시술이 유문부 경련을 일시적으로 호전시키고 증상도 개선시킨다는 보고가 있다[16]. 이외에도 위 전기자극 치료(gastric electrical stimulation), peroral endoscopic pyloromyotomy, 수술적 치료 등이 있다. 본 증례에서는 침습적인 치료가 어려운 고령 환자를 불응성 위마비로 오인하여 보툴리눔 독소 전정부 주입법을 시행하였다[7]. 지금까지 진행된 무작위 대조 연구에서 보툴리눔 독소 주입법은 환자 증상과 위 배출능에 효과가 없다고 결론을 내리고 있다[17,18]. 그럼에도 불구하고 현재까지는 보툼리눔 독소 주입법에 대하여 치료 대상이나 주입 방법에 따른 효과 등이 확인되지 않은 부분이 있다. 보툴리눔 독소 주입법은 부작용이 적고 시술이 쉬운 치료 방법으로 앞으로는 보툴리눔 독소 주입법이 치료 효과를 나타낼 것으로 보이는 치료 대상, 보툴리눔 독소 주입 양, 주입 방법 등에 대한 여러 대규모, 다기관 무작위 대조 연구가 필요할 것으로 보인다.
결론적으로 기능성 소화불량증이나 과민성 장증후군 환자가 위내시경, 복부 전산화단층촬영에서 정상이라고 할지라도 환자가 고령이고 체중 감소 외에도 원인이 확인되지 않는 복통이 있다면 소장암을 의심하는 것이 필요하다. 저자들은 소장암이 위마비로 오인되어 진단이 늦어진 증례를 경험하여 문헌 고찰과 함께 보고하는 바이다.
Notes
No potential conflict of interest relevant to this article was reported.