ģ ė”
ė§ģ ģķģ ģ°źµ¬ģė ė¶źµ¬ķź³ ģģ§ ģ¼ģ¹ė ź²°ė” ģ ģ»ģ§ė ėŖ»ķģģ§ė§ ķ¬ė¦¬ģ½ė°ķ° ķģ¼ė”ė¦¬(Helicobacter pylori, H. pylori) ź°ģ¼ģ“ ģ¬ķź“ ģ§ķź³¼ ź“ź³ź° ģģ ź²ģ“ė¼ė ź²ģ ėė¦¬ ģė ¤ģ§ ģ“ģ¼źø° ģ¤ģ ķėģ“ė¤. H. pylori ź°ģ¼ź³¼ ģ¬ķź“ ģ§ķģ ģ°ź“ģ±ģ ėķ ģ°źµ¬ ź²°ź³¼ė źøģ ģ ģø ź²¬ķ“ģ ė¶ģ ģ ģø ź²¬ķ“ź° ė§ģź³ ģģ“ ėŖ
ķķ ź²°ė” ģ ė“źø°ė ķė ģķģ“ė©°, ė§ģ ģķģ°źµ¬ģģ ģ¬ė¬ ė³ģøė” ģ“ ģ ģėź³ ģģ§ė§ ė¤ģķ źµė ė³ģģ ėķ ģģ ķ ė°°ģ ź° ģ“ė£Øģ“ģ§ģ§ ģź³ ė³ģøė” ģ ė·ė°ģ¹Øķ ģ ģė ģ¦ź±°ė¤ģ“ ģģ§ ė¶ģ”±ķ ģ¤ģ ģ“ė¤. ė³øź³ ģģė H. pylori ź°ģ¼ź³¼ ģ¬ķź“ ģ§ķģ ģ°ź“ģ±ģ ķģ¬ź¹ģ§ ėģØ ė¬øķ ź³ ģ°°ģ ķµķģ¬ ģ ė¦¬ķ“ė³“ź³ ģ ķė¤.
ė³ø ė”
1. H. pylori ģ ź“ģėė§„ ģ§ķ
1) ģµź·¼ź¹ģ§ģ ģ°źµ¬ ėķ„
1994ė
Mendall ė±[1]ģ“ H. pylori ź°ģ¼ź³¼ ź“ģėė§„ ģ§ķ(coronary artery disease, CAD)ģ ź“ė Øģ±ģ ėķģ¬ ģ²ģ ģ ģķ ģ“ķ ė§ģ ģ°źµ¬ė¤ģ“ ģ§ķėģ“ ģė¤. H. pylori ź°ģ¼ź³¼ CAD ė°ģź³¼ģ ģ°ź“ģ±ģ ģ“ķ“ė³ø ģ°źµ¬[2-21]ė ģģ ź° ģ°ź“ģ“ ģė¤ź³ ė³“ź³ ķ ģ°źµ¬[4-6,9,10,13-15,17-21]ģ ģģ ź° ģ°ź“ģ“ ģė¤ź³ ė³“ź³ ķ ģ°źµ¬[2,3,7,8,11,12,16]ź° ė§ģź³ ģģ¼ė©° ģģ§ź¹ģ§ ėŖ
ķķ ź²°ė” ģ ėģ¶ķģ§ ėŖ»ķź³ ģė¤(Table 1). ģ“ė¬ķ ģ“ģ ė ģ°źµ¬ ė°©ė² ė° ģ°źµ¬ ėģģ ģ“ģ§ģ± ėė¬øģ¼ė” ģź°ėė©°, źµė ė³ģė„¼ ė°°ģ ķģėģ§, ģ°źµ¬ ėģģ“ ź±“ź°ģøģøģ§ ģ¬ģ„ ģ§ķ ķģģøģ§ ė±ģ ė°ė¼ ź²°ź³¼ź° ė¤ė„“ź² ėķė ź°ė„ģ±ģ“ ģė¤[22,23].
ģµź·¼ģ ė©ķė¶ģģģė ź“ģėė§„ ģ”°ģģ ė” ģ§ėØė CADģ H. pylori ź°ģ¼ ź°ģ ģź“ģ±ģ ė³“ź³ ķģėė°, H. pyloriģ ź°ģ¼ėģģ ź²½ģ° CADģ ģķėź° ė ėģė¤(OR: 1.42, 95% CI: 1.09~1.86; P =0.008). ģ“ė¬ķ ķģģ 60ģø ėÆøė§ģ ģøźµ¬ģģ ė ėė ·ķģź³ ģ ė½ź³¼ ėÆøźµģ ģ°źµ¬ģģ ė ģ ģķ ģź“ģ±ģ ė³“ģ¬ ėģ“ģ ģøģ¢
ģ“ ź“ź³ź° ģė ź²ģ¼ė” ėķė¬ė¤[18]. ė¤ė„ø ė©ķė¶ģģģė CAD ė° ģ¬ź·¼ź²½ģź³¼ H. pylori ź°ģ¼ģ ģ°ź“ źµģ°Øė¹ė 2.53 (95% CI: 1.37~4.67)ģ“ģģ¼ė©° ķµź³ģ ģ¼ė” ģ ģķ ģėÆøź° ģģė¤[19]. H. pyloriģ CADź³¼ģ ź“ź³ģ ėķ ģµź·¼ģ ėė§ ģ°źµ¬ģģė ģ ź· ģ¹ė£ė„¼ ģķķ źµ°ģģ CADģģ ź“ė Øģ± ź°ģ(2.58% vs. 3.35%; P=0.09), CAD ź“ė Ø ģ¬ė§ė„ ģ ģ ķ(2.86% vs. 4.43%; P <0.01)ė„¼ ė³“ģ¬ģ£¼ģė¤[21]. ėķ, multidetector computed tomographyė” ģø”ģ ķ ź“ģėė§„ź²½ķģ¦ź³¼ H. pylori ź°ģ¼ ģģ±źµ°ź³¼ģ ģ°ź“ģ±ģ“ ė³“ź³ ėźø°ė ķģė¤(OR: 2.18, 95% CI: 1.051~7.528; P=0.04) (Table 1)[20].
Cytotoxin-associated gene A (CagA) ģģ± H. pylori ź· ģ£¼ģ CADģ ź“ė Øģ±ģ ėķ ģ°źµ¬ė¤ė ė§ģ“ ģ“ė£Øģ“ģ”ė¤. ķģ¬ź¹ģ§ģ ģ°źµ¬ ź²°ź³¼ė¤ģ ģ“ķ“ė³“ė©“ CagA ģģ± H. pylori ź°ģ¼ģ ģ¬ķź“ ģ§ķģ ģ“ķģØģ ķģ ķ ģ¦ź°ģķ¤ė ź²ģ¼ė” ė³“ģøė¤[24]. ģ¬ź·¼ź²½ģ ķģ, ė¶ģģ ķģ¬ģ¦ ķģģģ CagA ģģ± H. pylori ź°ģ¼ė„ ģ“ ėģ”°źµ°ģ ė¹ķģ¬ ķģ ķ ėģė¤ė ģ°źµ¬ ź²°ź³¼ź° ģė¤(ģ¬ź·¼ź²½ģ 86.7%, ė¶ģģ ķģ¬ģ¦ 91.7%, ėģ”°źµ° 58.3%)[25]. ė ė¤ė„ø ģ°źµ¬ģģė ź“ģėė§„ź²½ķź° ģė ķģźµ°ģģ CagA ķģ²“ź° ģė±ķ ėź² ģø”ģ ėģģ¼ė©°, CagA ķģ²“ģ ģź°ź° ėģģė” ėė§„ź²½ķ ķź“ģ źøøģ“ź° źøøģė¤ė ź²ģ“ ķ¹ģ“ķ ė§ķ ģ ģ“ģė¤[26]. Huang ė±[27]ģ CagA ģģ± H. pyloriģ ź°ģ¼ėģģ ė CRP, ģ“ģ½ė ģ¤ķ
ė”¤, ģ ė°ėģ§ģ§ėØė°±ģ§, ģ°ķė ģ ė°ėģ§ģ§ėØė°± ź·øė¦¬ź³ ģķ¬ģ§ģ§ėØė°±ģ§ģ“ CagA ģģ± H. pylori ģ ź°ģ¼ė ź²½ģ°ģ ė¹ķģ¬ ģ ģķź² ģ¦ź°ėė¤ź³ ė³“ź³ ķģė¤. ķģ§ė§ CagA ģģ± H. pylori ź°ģ¼ģ“ ģ¬ķź“ ģ§ķģ ģķģøģģģ ė°ķģ§ ėŖ»ķ ģ°źµ¬ė¤[7,16,28,29]ė ģģ“ ģ“ ģģ ģ¼ģ¹ė ź²°ė” ģ ėģ¶ķģ§ ėŖ»ķź³ ģė¤. ķģ¬ź¹ģ§ģ ģ°źµ¬ė„¼ ģ¢
ķ©ķ“ė³“ė©“ CagA ģģ± H. pylori ź°ģ¼ģ“ ķģ ķģ±ģ ģ ėķģ¬ ėė§„ź²½ķź° ķØģ¬ ė ģ¼ģ“ėźø° ģ¬ģ“ķź²½ģ ģ”°ģ±ķė ź²ģ¼ė” ģź°ėė¤[22,24] H. pylori ģ ź· ģ¹ė£ ķ CADģ ķøģ ģ¬ė¶ė„¼ ź“ģ°°ķ ģ°źµ¬ģģė ķź“ė“ė§ źø°ė„ģ ź°ģ [30] ė° ģ¬ė°ģ“ ģ¤ģė¤ė ģ°źµ¬ ė³“ź³ [31]ź° ģė ė°ė©“ CADģ ģ¬ė°ģ ķ° ģ°Øģ“ź° ģė¤ė ģ°źµ¬ ė³“ź³ ė ģė¤[32].
ģ¬ė§ė„ ź³¼ ź“ė Øķ“ģė ģµź·¼ģ ė©ķė¶ģģ ė°ė„“ė©“ ź±“ź°ķ ė¬“ģ¦ģ ķ¼ķģģģ H. pylori ģ ź· ģ¹ė£ė ģ ģ¬ė§ė„ ź°ģģ ź“ė Øģ“ ģģ§ė§ ģ ė°ģ ģø ģ¬ė§ė„ ģ ģ¦ź° ź²½ķ„ģ ė³“ģ“ė ź²ģ¼ė” ė³“ź³ ėģė¤[33]. ź·øė¬ė Kim ė±[34]ģ ź³ ķģ ģ¹ė£ ķģė„¼ ķ¬ķØķ źµėƼź±“ź°ė³“ķ ė°ģ“ķ°ė² ģ“ģ¤ė„¼ ģ“ģ©ķ ģøźµ¬ źø°ė° ģ°źµ¬ģģ ė¤ė„ø ź²°ź³¼ė„¼ ė³“ź³ ķģė¤. H. pylori ģ ź· ģ¹ė£ė„¼ ė°ģ 5,541ėŖ
ģ ķģģ ģ ź· ģ¹ė£ė„¼ ė°ģ§ ģģ 1,182ėŖ
ķģģ ģ¬ė§ė„ ģ ė¹źµķģģ ė, ģ ģ²“ ģ¬ė§ė„ ź°ģ(hazard ratio: 0.70, 95% CI: 0.60~0.82) ėė ėķź“ ģ¬ė§ė„ (hazard ratio: 0.46, 95% CI: 0.26~0.81)ģ ź°ģė„¼ ėķėģ¼ė ė°ėė” ģ¬ķź“ ģ§ķģ¼ė” ģøķ ģ¬ė§ė„ ģ ģ°Øģ“ź° ģģė¤[34].
2) ģ¬ķź“ ģ§ķź³¼ ģ°ź“ė ė³ķģė¦¬
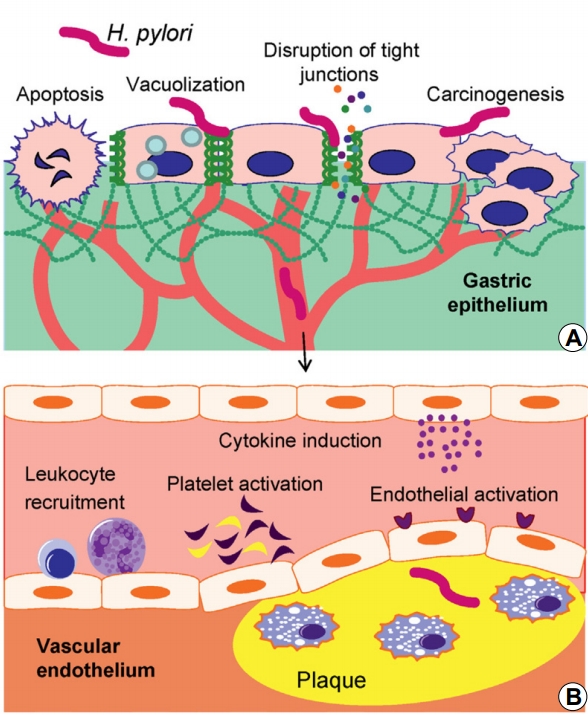
H. pyloriė ķģ” ė“ģ ėØķµźµ¬ė„¼ ģź·¹ķģ¬ ķģ” ģź³ ė„¼ ģ ė°ģķ¬ ģ ģģ¼ė©°, von Willebrand factor ķģģ H. pylori ź°ģ¼ź³¼ ź°ķ ģź“ģ±ģ“ ģė¤. H. pyloriė plasminogen activator inhibitor-1ģ ė°ķģ ģź·¹ķź³ ķģķģ ķģ± ė° ģģ§ģ ģ¼ģ¼ķ¤ė©°, ģ¤ģ±ģ§ė°© ė° ė¤ģķ ėė§„ź²½ķģøģė„¼ ģ¦ź°ģķØė¤. ėķ, H. pyloriė ķģ² tumor necrosis factor-alpha ģģ¹ ģģ¹ź³¼ ģ°ź“ģ“ ģė¤[35]. ė§ģ± H. pylori ź°ģ¼ ģķģģė ģ ė±źøģ źøģ±ģ¼ģ¦ ė°ģź³¼ ķ¼ėøė¦¬ė
øź²(fibrinogen)ź³¼ ź°ģ źøģ±źø° ģź³ ėØė°±ģ§ģ“ ģ¦ź°ėė¤. ģ“ė¬ķ źø°ģ ģ ķµķģ¬ źøģ± ķģ ģ± ķź“ ģ§ķģ“ ė°ģķ ģ ģėė° fibrinogenģ H. pylori ź°ģ¼ź³¼ ė§¤ģ° ģ°ź“ģ“ ģė ź²ģ¼ė” ė³“ź³ ėź³ ģė¤[36]. ėķ, ė§ģ± ģ¼ģ¦ ģķģģė ź“ė Øė ģ¬ģ“ķ ģ¹“ģø ė±ģ“ ė¶ė¹ėź³ ģ“ ģķ„ģ¼ė” ķģ¤ ģ§ģ§ ģ”°ģ± ė³ķ, ķģ” ģź³ ģ²“ź³ģ ķģ±ķ, ķģķ ģģ§ ģ ė ė° ķź“ ė“ķ¼ģøµģ ģģģ ģ ė°ķģ¬ ėė§„ź²½ķź° ė ģ ģ ė°ėė ź²ģ¼ė” ģź°ķź³ ģė¤(Fig. 1)[22,36,37].
2. H. pylori ģ ėķź“ ģ§ķ
ėė§„ź²½ķģ ģ ė°ģøģė”ģ H. pylori ź°ģ¼ģ“ ģ°źµ¬ėė©“ģ ķķģ± ėķź“ ģ§ķź³¼ H. pylori ź°ģ¼ģ ģ°ź“ģ±ė ģ°źµ¬ėģė¤. ź³¼ź±°ģ ģķė ģ¼ė¶ ģź·ėŖØ ģ°źµ¬ģģė H. pylori ź°ģ¼ģ“ ėė§„ź²½ķģ ģ°ź“ė ėÆøģøķź“ė³ ģ¤ ėķź“ ģ§ķź³¼ ź“ė Øģ“ ģė¤ź³ ķģģ¼ė[38-42] ėź·ėŖØ ģ°źµ¬ģģė H. pylori ź°ģ¼ģ“ ķķģ± ėķź“ ģ§ķź³¼ ģ°ź“ģ“ ģź±°ė ģ½ź° ģķ„ģ“ ģė ģ ėė” ė°ķģ”ė¤[5]. CagA ģģ± H. pyloriź° ķķģ± ėķź“ ģ§ķģ ė³ķģė¦¬ģ ėÆøģ¹ė ģķ„ģ ėķ“ģė ė³“ź³ ė ė° ģėė°, Diomedi ė±[43]ģ ė°ė„“ė©“ CagA ģģ± H. pylori ź°ģ¼ģ“ ģė ź²½ģ° ķķģ± ėķź“ ģ§ķģ ģ¬ė°ė„ ģ“ ģė±ģ“ ėģė¤ė ź²ģ“ ė°ķģ”ė¤. ėķ, 10ź°ģ ķģ-ėģ”°źµ° ģ°źµ¬ė„¼ ė¶ģķ ė©ķė¶ģģģė CagA ģģ± H. pyloriģ ź°ģ¼ė ź²½ģ° CagA ģģ± H. pylori ź°ģ¼źµ°ė³“ė¤ ķķģ± ėķź“ ģ§ķģ ģķėź° 2.66ė°° ėė¤ź³ ė³“ź³ ķģė¤[13]. ė ė¤ė„ø ė©ķė¶ģģģė H. pylori CagA ķģ² ģģ±ģ ķķģ± ėģ”øģ¤ģ ģķź³¼ ė°ģ ķ ź“ė Øģ“ ģģ“ CagA ķģ² ģģ±ģ ė¤ė„ø ģ§ėØ ėźµ¬ė³“ė¤ ėģ”øģ¤ģ ģķģ ė³“ė¤ ķØź³¼ģ ģ¼ė” ģģø”ķ ģ ģė¤ź³ ė³“ź³ ķģė¤[44]. ķģ§ė§ ģ ķ„ģ ģ½ķøķø ģ°źµ¬ģģė ė¤ė„ø ź²°ź³¼ź° ėģ¶ėģė¤. ėÆøźµģøģ ėģģ¼ė” ģķė ģ ķ„ģ ģ½ķøķø ģ°źµ¬ģģė H. pylori ģģ±źµ°ģģ ķķģ± ėģ§ķģ ORė„¼ 1.13 (95% CI: 0.68~1.89)ģ¼ė” ė³“ź³ ķģģ¼ė, ģ“ ģ°źµ¬ģģė CagA ź· ģ£¼ģ ėģ”øģ¤ģ ģķģ ź³ ė ¤ķģ§ ģģ ėØģ ģ“ ģė¤[45]. ESTHER ģ½ķøķøė„¼ ģ“ģ©ķ ė ė¤ė„ø ģ ķ„ģ ģ°źµ¬ģģė ėģ”øģ¤ ģķ, H. pylori ķģ² ģģ± ė° CagA ķģ² ģģ± ģ¬ģ“ģ ģ°ź“ģ±ģ ģ”°ģ¬ķģģ¼ė CagA ģģ± ėė CagA ģģ± H. pyloriė ėģ”øģ¤ ģķģ ģģø”ķØź³¼ź° ģģė¤[16].
3. H. pylori ģ ė¶ģ ė§„
H. pylori ź°ģ¼ź³¼ ģ¬ģ„ ė¶ģ ė§„ģ ź“ź³ė 1998ė
ģ²ģ ģ ģėģź³ , ė¹ģ Frustaci ė±[46]ģ ģ¼ģ¦ģ ģķ ģ¬ė°© źµ¬ģ”° ė³ķė„¼ ģ ģķģ¬ ģ¬ė°©ģøė(atrial fibrillation, AF)ź³¼ ģ¼ģ¦ ė°ģģ“ ź“ź³ź° ģģģ ė°ķķģė¤. 2001ė
ģ Chung ė±[47]ģ AFģ ķģ” ė“ ģ¼ģ¦ģøģģģ ź“ė Øģ±ģ ėķģ¬ ė°ķķ ģ“ķ, 2005ė
Montenero ė±[48]ģ AF ķģģģ ėģ”°źµ°ė³“ė¤ H. pylori ķģ²“ ė° CRPź° ėģģ ģ¦ėŖ
ķģ¬ H. pylori ź°ģ¼ģ“ AFģ ģģøģ“ ė ģ ģģģ ģ ģķģė¤. ģ“ė¤ģ ģģøķ¬ģ ģģ±ģķķģø H+/K+-ATPaseģ ģ¬ģ„ģøķ¬ģ ķķģø Na+/K+-ATPase ź°ģ ģ ģ¬ģ±ģ“ ģė¤ė ģ ģ ź³ ė ¤ķģ¬ H. pylori ź°ģ¼ģė¤ģ ģ¼ė¶ģģ ź“ģ°°ėė ģė²½ģøķ¬ģ ģź°ķģ²“ź° ģ¬ģ„ģ ATP ź°ģė¶ķ“ė„¼ ģ ķ“ķØģ¼ė” ģ“ģØģ ķģģ±ģ ė¶ź· ķģ ģ“ėķģ¬ ģ¬ė°©ģøėģ ģ“ėķģģ ź²ģ“ė¼ė źø°ģ ģ ģ ģķģė¤[48]. ģ“ķ H. pylori ź°ģ¼ź³¼ ė¶ģ ė§„, ķ¹ķ ģ¬ė°©ģøėź³¼ģ ź“ź³ė„¼ ģ“ķ“ė³ø ģ¬ė¬ ģ°źµ¬ź° ģģģ§ė§ H. pylori ź°ģ¼ģ“ ģ¬ė°©ģøėź³¼ ģ°ź“ģ“ ģź³ ģ¬ė°©ģøėģ ė°ģģ ģķ„ģ ėÆøģ¹ė¤ė ģ°źµ¬ź° ģė ė°ė©“, ģ¬ė°©ģøėź³¼ė ź“ė Øģ“ ģė¤ė ģ°źµ¬ė ģģ“ ģģ§ź¹ģ§ ģ¼ģ¹ė ź²°ź³¼ė„¼ ė³“ģ“ģ§ ėŖ»ķź³ ģė¤(Table 2)[48-55]. ģµź·¼ Tetta ė±[56]ģ ģ¬ė°©ģøėź³¼ ź“ė Øķģ¬ 6ź°ģ ķķ„ģ ź“ģ°° ģ°źµ¬ė„¼ ķ¬ķØķ ė©ķė¶ģģ ģķķģģ¼ė H. pylori ģ ė³ė„ ģ AF ź·øė£¹ź³¼ ė¹AF ź·øė£¹(ź°ź° 35.0% ė° 32.7%) ģ¬ģ“ģ ģ°Øģ“ź° ģģė¤.
ź²° ė”
H. pylori ģ ģ¬ķź“ ģ§ķģ ģ°ź“ģ±ģ ėķ“ģė ģģ§ė ė
¼ėģ“ ģė¤. ģ¬ķź“ ģ§ķ ė°ģģ ģķ„ģ ģ£¼ė ģķģøģė ė§¤ģ° ė¤ģķģ¬ ė³“ģ ķģ¬ ė¶ģķźø°ģė ģ“ė ¤ģ“ ģ ģ“ ė§ė¤. ė§ģ ģ°źµ¬ģģ ź²°ź³¼ė¤ģ“ ģ¼ģ¹ķģ§ ģė ź²ģ ė³“ģ ķ“ģ¼ ķ źµė ė³ģė¤ģ“ ėė¬“ ė§ź³ ė³µģ”ķė¤ė ģ ģ źø°ģøķė¤. ķģ¬ź¹ģ§ģ ź·¼ź±°ė”ė H. pylori ė ė§ģ± ģ¼ģ¦ ė°ģģ ķµķģ¬ ėė§„ź²½ķģ źø°ģ ģ ź“ģ¬ķė©°, ķ¹ķ CagA ģģ± H. pylori ź· ģ£¼ė ķģ ķģ±ģ ģ ėķģ¬ ėė§„ź²½ķė„¼ ķØģ¬ ė ģ ģ¼ģ¼ķ¬ ģ ģė¤ė ź²ģ“ė¤. ģ°ė¦¬ėė¼ė H. pylori ź°ģ¼ź³¼ ģ¬ķź“ ģ§ķ ė ź°ģ§ģ ģ ė³ė„ ģ“ ėŖØė ėģ¼ėÆė” ģ“ė¤ģ ģ°ź“ģ±ģ ź·ėŖ
ķė ź²ģ ģ§ė³ģ ģė°© ė° ģ¹ė£ė„¼ ģķģ¬ ė§¤ģ° ģėÆø ģė ģ¼ģ“ė¼ ķ ģ ģź² ė¤. ė°ė¼ģ ķ„ķ H. pylori ģ ģ¬ķź“ ģ§ķģ ģøź³¼ź“ź³ė„¼ ź·ėŖ
ķźø° ģķ“ģė ģ ķ„ģ ģø ėź·ėŖØ ė¬“ģģ ģ°źµ¬ ė° H. pylori ģ ź· ģ¹ė£ź° ģ¬ķź“ ģ§ķģ ģė°©ģ ģ“ė¤ ģķ„ģ ėÆøģ¹ėģ§ģ ėķ ģ ķ„ģ ė¬“ģģ ģ¤ģ¬ ģ¤ķ ģ°źµ¬ź° ķģķ ź²ģ¼ė” ģ¬ė£ėė¤.