조기위장관암 내시경 치료 임상진료지침
Clinical Practice Guideline for Endoscopic Resection of Early Gastrointestinal Cancer
Article information
 , Dong-Hoon Yang2,*, Jong Wook Kim3, Jie-Hyun Kim4, Ji Hyun Kim5, Yang Won Min6, Si Hyung Lee7, Jung Ho Bae8, Hyunsoo Chung9, Kee Don Choi2, Jun Chul Park10, Hyuk Lee6, Min-Seob Kwak11, Bun Kim12, Hyun Jung Lee9, Hye Seung Lee13, Miyoung Choi14, Dong-Ah Park14, Jong Yeul Lee,15,**, Jeong-Sik Byeon,2,**, Chan Guk Park16, Joo Young Cho17, Soo Teik Lee18, Hoon Jai Chun19
, Dong-Hoon Yang2,*, Jong Wook Kim3, Jie-Hyun Kim4, Ji Hyun Kim5, Yang Won Min6, Si Hyung Lee7, Jung Ho Bae8, Hyunsoo Chung9, Kee Don Choi2, Jun Chul Park10, Hyuk Lee6, Min-Seob Kwak11, Bun Kim12, Hyun Jung Lee9, Hye Seung Lee13, Miyoung Choi14, Dong-Ah Park14, Jong Yeul Lee,15,**, Jeong-Sik Byeon,2,**, Chan Guk Park16, Joo Young Cho17, Soo Teik Lee18, Hoon Jai Chun19
Trans Abstract
Although surgery was the standard treatment for early gastrointestinal cancers, endoscopic resection is now a standard treatment for early gastrointestinal cancers without regional lymph node metastasis. High-definition white light endoscopy, chromoendoscopy, and image-enhanced endoscopy such as narrow band imaging are performed to assess the edge and depth of early gastrointestinal cancers for delineation of resection boundaries and prediction of the possibility of lymph node metastasis before the decision of endoscopic resection. Endoscopic mucosal resection and/or endoscopic submucosal dissection can be performed to remove early gastrointestinal cancers completely by en bloc fashion. Histopathological evaluation should be carefully made to investigate the presence of risk factors for lymph node metastasis such as depth of cancer invasion and lymphovascular invasion. Additional treatment such as radical surgery with regional lymphadenectomy should be considered if the endoscopically resected specimen shows risk factors for lymph node metastasis. This is the first Korean clinical practice guideline for endoscopic resection of early gastrointestinal cancer. This guideline was developed by using mainly de novo methods and encompasses endoscopic management of superficial esophageal squamous cell carcinoma, early gastric cancer, and early colorectal cancer. This guideline will be revised as new data on early gastrointestinal cancer are collected.
서론
내시경 절제술은 조기식도암, 조기위암, 조기대장암 등 조기위장관암의 치료를 위한 최소 침습 수술법이다[1]. 국내에서는 건강검진 목적의 상부위장관내시경 및 대장내시경 검사가 널리 시행되면서 위장관암의 조기 진단 비율이 늘고 있고, 이에 따라 조기위장관암의 내시경 절제술 건수 역시 증가하고 있다[2,3]. 특히 내시경 절제술 중 내시경 점막하 박리술은 병변의 크기 및 위치와 상관 없이 일괄 절제가 가능하다는 장점으로 인하여 시술 건수가 빠르게 늘어 현재 연간 수천 건 이상이 시술되고 있다[3,4]. 내시경 점막하 박리술은 1999년에 국내에 소개된 이후 2003년부터 조기위암의 치료로 널리 받아들여지기 시작하였는데, 2014년에는 국내의 45개 3차 의료기관 모두에서 내시경 점막하 박리술을 시행하였고, 287개 종합병원의 44%인 125개 종합병원에서 내시경 점막하 박리술을 시행하는 등 전국적으로 시술이 이루어지고 있다[5].
내시경 절제술은 전신마취 없이도 시행할 수 있고, 수술적 절제에 비하여 회복이 빠르고 재원 기간이 짧으며 비용이 적게든다는 장점이 있다[6]. 하지만 내시경 절제술은 림프절을 절제할 수 없고 원발 국소 병변만 절제하기 때문에 내시경 절제술을 시행하기에 앞서 림프절 전이가 없을 것으로 생각되는 조기위장관암 환자를 선별하는 것이 중요하다[1,7,8]. 또한, 내시경 절제술로 국소 절제가 잘 이루어졌다 하더라도 병리검사에서 림프절 재발과 연관되는 위험인자가 발견된 경우에는 암 재발과 전이의 가능성을 최소화하기 위하여 외과적 절제 수술을 고려해야 한다. 이러한 임상적 결정에 고해상도 내시경, 영상강화내시경, 색소내시경(chromoendoscopy), 확대내시경, 초음파내시경, 컴퓨터단층촬영 등 다양한 영상검사를 활용하려는 노력이 있고[9-15], 림프절 전이 가능성이 높은 환자를 예측하는 여러 모델이 개발되었다[1,7,8,16,17]. 이러한 연구 결과를 바탕으로 임상의의 진료 및 치료 방침 결정에 도움을 줄 수 있는 국외 진료지침이 발표된 바도 있다[1]. 하지만 조기위장관암의 발생 빈도는 표적 장기(식도, 위, 대장 등) 및 국가와 지역에 따라 큰 차이가 있고, 임상에서 이용 가능한 시술 도구 및 방법, 가용한 의료 자원도 동일하지 않다. 따라서, 국외에서 개발된 조기위장관암에 대한 내시경 절제술 임상진료지침을 국내 의료 환경에 그대로 적용하는 것은 적절하지 않다. 그럼에도 불구하고, 아직까지 조기위장관암의 내시경 절제술에 관한 국내 임상진료지침이 개발되어 있지 않아, 국내 내시경 의사들은 국외 임상진료지침을 참고하거나 국내에서 이루어진 개별 연구들을 직접 검토하여 진료에 활용해야 하는 불편함이 있었다. 이 임상진료지침에서는 조기위장관암에 대한 내시경 절제술 관련 국내외 연구들을 종합적으로 검토하고, 국내의 조기위장관암 역학적 특성과 임상 양상, 의료 환경을 감안하여 조기위장관암 환자의 진료 및 치료에 참고할 수 있는 권고안을 개발하고자 하였다. 조기위장관암 진료에 대한 이 임상진료지침은 표재성 식도편평상피암, 조기위암, 조기대장암의 세 부분으로 이루어져 있으며, 앞으로 새로운 국내외 연구 결과에 따라 보완, 개정되어야 할 것이다.
방법
1. 진료지침 개발의 목적과 범위
현재까지 제시된 국내외의 근거를 기반으로 국내 의료 실정에 부합하고 임상적으로 수행 가능한 조기위장관암의 내시경 절제술 진료지침을 개발하고자 하였다. 이 지침은 내시경 절제술 적용이 가능한 표재성 식도편평상피암, 조기위암, 조기대장암 성인 남녀 환자를 대상 인구집단으로 한다. 이 임상진료지침 사용 대상자는 1차, 2차, 3차 의료기관에서 소화기내시경 검사 및 시술을 시행하는 소화기내과 의사이며, 내시경 절제술 관련 용어에 대한 정의는 Table 1에 제시하였다. 이 임상진료지침은 조기위장관암 환자의 진단 및 내시경 절제술 전 평가, 내시경 절제술 방법의 선택, 내시경 절제술 후 관리에 있어 적정 진료를 위한 의사 결정을 하는데 있어 도움을 주고자 하였다. 또한, 전공의 및 병원 근무 인력에 대해서도 진료의 길잡이 역할을 하고자 하며, 아울러 환자와 일반인에 대해서도 실제적이고 표준적인 의학 정보를 제공하고자 하였다.

Definition of Terms Related to Endoscopic Resection
2. 임상진료지침 위원회 구성 및 개발 과정
임상진료지침 운영위원회는 대한소화기내시경학회 전훈재 이사장, 이수택 회장 및 임원진을 중심으로 2017년 11월에 구성되어 진료지침 개발 전략을 수립하고 관련 위원장을 선임하였으며, 사업 관련 예산을 검토 및 승인하였다. 또한, 권고사항을 검토하고 지침의 개정에 관하여 이해당사자의 참여 및 편집의 독립성이 적절히 유지되고 있는지에 대하여 검토 및 감독하였다. 최종 지침의 검토 및 출판은 2020년 1월 대한소화기내시경학회 조주영 이사장, 박찬국 회장 및 임원진으로 이루어진 임상진료지침 운영위원회에서 승인하였다.
임상진료지침 운영위원회는 대한소화기내시경학회 진료지침 TF (Korean Society of Gastrointestinal Endoscopy Task Force on Clinical Practice Guideline)를 구성하였으며, 대한소화기내시경학회 진료지침 TF는 임상진료지침 개발위원회로서 조기위장관암의 내시경 절제술에 관한 임상진료지침 개발을 총괄 및 감독하였다. 임상진료지침의 다학제 개발을 위하여 대한소화기내시경학회 소속 소화기내과 전문의 변정식을 개발위원회 위원장으로 하여, 대한소화기내시경학회(김정욱, 김지현, 김지현, 민양원, 박찬혁, 이시형, 이종열), 대한소화기학회(배정호, 양동훈, 정현수, 최기돈), 대한상부위장관·헬리코박터학회(박준철, 이혁), 대한장연구학회(곽민섭), 대한소화기암학회(김번, 이현정), 대한병리학회(이혜승)에서 추천된 소화기내과 및 병리과 전문의가 개발위원회 위원으로 참여하였다. 또한, 한국보건의료연구원 소속 임상진료지침 개발 방법론 전문가 2인(박동아, 최미영)도 개발위원회 위원으로 참여하였다. 조기위장관암의 분야별 체계적 임상진료지침 개발을 위하여 표재성 식도편평상피암(팀장: 최기돈), 조기위암(팀장: 이종열), 조기대장암(팀장: 양동훈) 소위원회가 구성되었다. 개발 소위원회는 진료지침의 핵심 질문 선정, 문헌 검색, 권고안 도출, 진료지침 초고 작성과 수정을 진행하였다.
개발 소위원회 사이의 개발 과정 통일성 유지를 위하여 개발위원회는 2017년 12월 22일부터 총 4회의 임상진료지침 개발위원회 회의를 진행하였으며, 임상진료지침 개발 방법론 확립과 개발 과정 검토를 위하여 총 2회의 워크숍을 개최하였고, 개발 방법론, 근거 및 권고등급 부여와 권고문 합의 방법에 관한 교육을 병행하였다(2018년 3월 12일, 2018년 11월 10일). 개발 위원회는 본 지침의 권고안을 de novo 방식으로 개발하기로 결정하였고, 개발 소위원회는 다수의 온라인 및 대면 회의를 통하여 진료지침 개발을 진행하였다.
3. 핵심 질문 선정
진료지침에 포함할 핵심 질문을 도출하기 위하여 PICO 원칙하에 선정기준을 정하고 조사표를 설계하였다. P (population)는 표재성 식도편평상피암, 조기위암, 조기대장암 환자, I (intervention)는 진단법 혹은 치료법을 포함한 중재, C (comparison)는 특정 중재법과 비교가 되는 비교군, O (outcome)는 진단의 유용성 혹은 치료 결과이다. PICO 원칙하 선정 과정을 Supplementary Material I에 제시하였다. 핵심 질문 초안을 요약한 조사표를 취합하여 개발 소위원회 위원 간 토의로 우선순위를 정하여 진료지침에 포함할 핵심 질문을 선정하였다. 제외기준으로는 사람을 대상으로 한 연구가 아닌 경우, 핵심 질문의 관심 환자를 대상으로 하지 않은 경우, 핵심 질문 관련 중재 및 비교중재가 시행되지 않은 경우, 종설, 증례보고, 초록으로만 발표된 연구, 영어나 한국어로 출판되지 않은 연구, 원문을 구할 수 없는 연구를 포함하였고, 개별 연구 간 대상 집단이 중복되는 경우에는 더 작은 규모의 연구를 배제하였다.
4. 문헌 검색 및 선택
2018년 8월에 MEDLINE, EMBASE, Cochrane Library, KoreaMed 및 Guideline International Network를 이용하여 핵심 질문에 따른 문헌 검색을 시행하였다. 검색 색인단어는 식도암 관련 색인단어((“esophageal” OR “esophagus” OR “oesophageal” OR “oesophagus” OR “gullet”) AND (“cancer$” OR “tumo?r” OR “carcinoma$” OR “adenocarcinoma$” OR “neoplas$”)), 위암 관련 색인단어((“stomach” OR “gastric”) AND (“cancer$” OR “tumo?r” OR “carcinoma$” OR “adenocarcinoma$” OR “neoplas$”)), 대장암 관련 색인단어((“colon$” OR “rectum” OR “colorectal” OR “rectal”) AND (“polyp$” OR “cancer” OR “adenoma$” OR “adenocarcino$” OR “carcino$” OR “tumo?r”)), 내시경 절제술 관련 색인단어((“endoscop$”) AND (“dissection” OR “resection” OR “treat$” OR “ESD”))를 사용하였으며, 이 외 핵심 질문에 따라 검색 색인단어를 조정 및 조합하여 문헌을 검색하였다. 문헌 검색은 한국보건의료연구원 최미영 연구원이 시행하였으며, 검색원 간의 교차 검색에 따른 중복 문헌을 제외하였다. 핵심 질문별로 두 명의 개발위원을 배정하여 선정기준과 제외기준에 맞추어 독립적으로 문헌을 선택하였다. 일차적으로는 문헌의 제목과 초록을 보고 진료지침 개발에 적합하지 않은 문헌을 배제하였고, 제목과 초록만으로 배제되지 않은 문헌은 전문을 검토한 후 최종적으로 문헌 선택 또는 배제 여부를 결정하였다. 두 위원간 의견이 불일치하는 경우에는 의견 조율을 통하여 문헌 선택 여부를 결정하였고, 조율이 되지 않은 경우 개발 소위원회 팀장이 최종 결정하였다. 자세한 문헌 검색 과정은 Supplementary Material II에 제시하였다.
5. 문헌의 비뚤림 위험 평가와 근거 요약 및 권고등급
근거에 사용될 자료로 선택된 문헌에 대한 타당성 평가를 위하여 체계적이고 일관된 평가 방법을 사용하였다. 무작위 배정 비교 연구는 코크란의 최신 risk of bias법을 이용하여 평가하였고[18,19], 비무작위 연구의 평가는 RoBANS 2.0 및 Newcastle-Ottawa assessment scale을 이용하였다[20]. 진단 연구의 평가를 위해서는 QUADAS-2 도구를 사용하였다[21]. 근거 요약은 GRADE 방법을 이용하여 결정되었다[22]. 문헌의 연구 유형에 따라 무작위 배정 비교 연구는 높은 근거수준을, 관찰 연구는 낮은 근거수준을 기본으로 하되, 연구의 질에 영향을 주는 요소를 고려하여 해당 연구의 질적 수준을 올리거나 내려 근거수준을 높음(high), 중등도(moderate), 낮음(low), 매우 낮음(very low)과 같이 네 단계로 구분하였다.
권고의 등급은 바람직한 효과와 바람직하지 못한 효과의 균형, 근거의 질, 가치와 선호 등의 측면을 고려하여 강한 권고(strong recommendation)와 약한 권고(weak recommendation)로 구분하였다. 강한 권고는 특정 중재에 대하여 권고를 따를 경우 바람직한 효과가 바람직하지 않은 효과보다 크고, 근거의 질이 높으며, 다른 중재와 비교하여 가치와 선호도가 우수하기 때문에 대부분의 환자에서 시행할 것을 권하는 등급이다. 약한 권고란 효과 크기가 상대적으로 작거나 근거가 다소 약하지만 바람직한 효과가 있어 다수의 환자에서 시행되는 것이 좋을 것으로 판단되는 등급이다. 약한 권고 등급에서는 일부 환자에서 혹은 의료진의 가치나 선호도에 따라 다른 중재를 선택할 수 있다. 권고안 및 권고등급, 근거수준은 Table 2~4에 요약하여 정리하였다.

Summary and Strength of Recommendations for Superficial Esophageal Squamous Cell Carcinoma
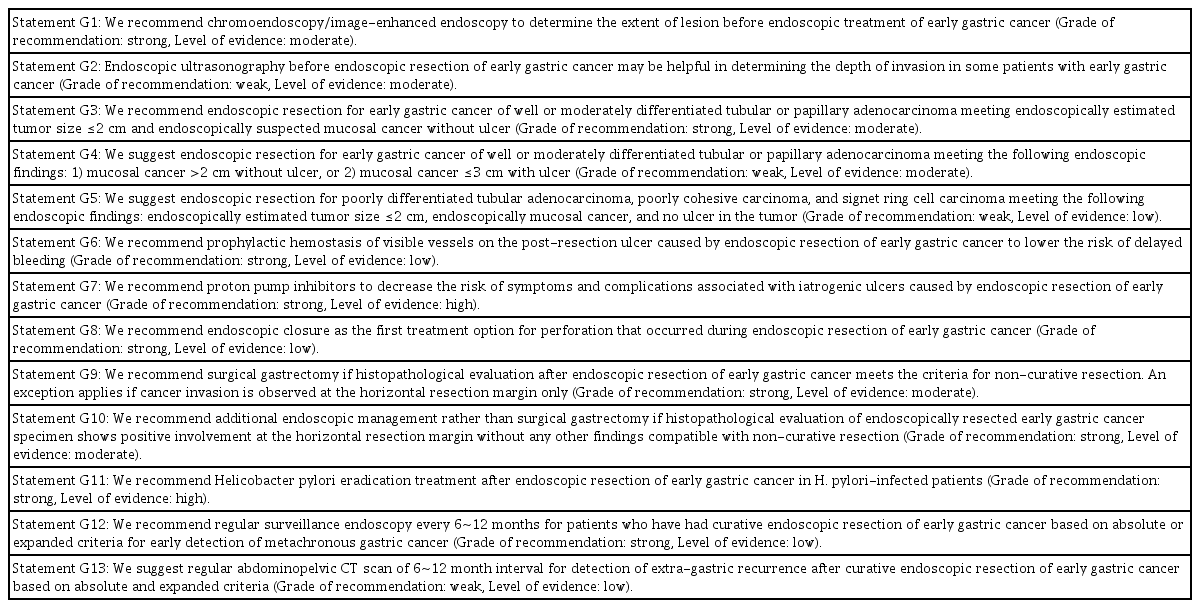
Summary and Strength of Recommendations for Early Gastric Cancer

Summary and Strength of Recommendations for Early Colorectal Cancer
6. 검토 및 승인
감수위원회는 2019년 8월에 대한소화기내시경학회 임원 29명과 보험위원회 위원 14명, 내시경점막하박리술연구회 위원 15명으로 구성되어 개방형 질문을 이용하여 초안 평가를 실시하였다. 지침의 미비한 부분은 개발위원회에서 수정 후 감수위원회의 재평가를 받아 진료지침의 균형성과 완결성을 높이고자 하였다. 외부 검토를 위하여 2019년 8월 18일 전국의 내시경 의사 및 간호사가 참여하는 제61회 대한소화기내시경학회 세미나에서 38명의 소화기내시경 전문가가 참여한 공청회를 개최하여 공개적으로 의견을 들었으며, 지적 사항을 최종 임상진료지침에 반영하였다.
7. 진료지침의 보급과 갱신 계획
이 임상진료지침의 보급 및 확산을 위하여 지침안을 Clinical Endoscopy 및 대한소화기학회지, 대한상부위장관·헬리코박터학회지, Intestinal Research, 대한소화기암학회지에 공동 게재하며, 대한소화기내시경학회 홈페이지에 게시하고, 임상진료지침정보센터에 등록하고자 한다. 다만, 임상진료지침의 데이터베이스 등록을 통한 수동적 확산은 일선에서 환자를 진료하는 내시경 의사에게 빠른 보급이 어려울 수 있을 것으로 예상되며, 이러한 장애 요인을 극복하기 위하여 주관 학회인 대한소화기내시경학회에서는 진료지침을 전자우편 등 다양한 형식으로 무료로 배포하고, 향후 다양한 소화기 관련 학술대회, 세미나, 워크숍 등을 통하여 적극적으로 홍보할 예정이다. 임상진료지침은 현재 개발을 진행하는 시점에서의 권고안으로, 향후 진료지침 권고안을 변경할 만한 중요한 연구가 새로이 축적되어 진료지침 개정이 필요하다고 판단되면 개정을 시행할 예정이다.
8. 지침의 한계
이 임상진료지침의 가장 중요한 한계점은 국내 근거가 충분하지 않다는 점이다. 국내의 근거가 부족한 경우에는 국외의 자료를 이용할 수 밖에 없는데, 국외의 자료는 우리나라와 조기위장관암의 역학적 특성, 임상 양상 등이 다르기 때문에 근거를 그대로 수용하기 어려운 경우가 있다. 또한, 이 임상진료지침은 실제 임상에서 의료진이 환자를 진료할 때 절대적인 진료 기준을 제시하고자 함이 아니고, 현재까지 밝혀진 과학적 근거를 바탕으로 일선에서 조기위장관암 진료를 담당하는 의사가 임상적 판단을 하는데 도움을 주기 위한 것이다. 따라서, 개개인의 환자에 대한 진료 행위는 담당 의사가 환자의 여러 임상적 요인을 고려하여 최종적으로 결정해야 한다. 이 임상진료지침은 실제 진료를 담당하는 의사의 의료 행위를 제한하는 목적이나 건강보험 심사의 기준으로 사용되어서는 안 되고, 또한 특정 환자에게 시행된 진료 행위에 대한 법률적 판단을 위하여 이용되어서도 안 된다.
9. 편집의 독립성
이 임상진료지침은 대한소화기내시경학회 사업으로 선정되어 대한소화기내시경학회로부터 재정 지원을 받았으나 재정 지원자가 지침을 개발하는 과정에 영향을 주지 않았고, 지침 개발과정에 참여한 모든 구성원은 지침 개발과 관련하여 이해관계나 잠재적인 이해상충이 없었다.
표재성 식도편평상피암
1. 권고안 E1: 표재성 식도편평상피암에서 원격 및 림프절 전이가 없고 명확한 점막하층 침범이 없을 경우 내시경 절제술 시행을 권고한다(권고등급: 강함, 근거수준: 중등도).
Statement E1: We recommend endoscopic resection for superficial esophageal squamous cell carcinoma (SESCC) without distant or lymph node metastasis, excluding those with obvious submucosal invasion (Grade of recommendation: strong, Level of evidence: moderate).
점막층이나 점막하층에 국한된 식도의 편평상피암을 표재성 식도편평상피암이라고 하는데 그중 원격 전이가 없고, 림프절 전이 가능성이 거의 없는 점막층에 국한된 표재성 식도편평상피암은 내시경 절제술의 좋은 대상이다. 표재성 식도편평상피암에 대한 내시경 절제술은 식도를 보존할 수 있다는 큰 장점이 있지만 표재성 식도편평상피암이라 하더라도 림프절 전이가 있을 수 있기 때문에 내시경 절제술의 대상 선정이 매우 중요하다. National Comprehensive Cancer Network 가이드라인은 표재성 식도편평상피암이 점막에 국한된 경우에는 내시경 절제술을, 점막하 침윤이 있는 경우에는 식도절제술 시행을 권고하고 있다[23]. 일본 식도암 연구회는 점막고유층까지만 침범한 점막암인 경우에 림프절 전이가 거의 없기 때문에 이를 내시경 절제술의 절대 적응증으로 정의하였다[17]. 유럽내시경학회 가이드라인에서도 림프절 전이가 없고 점막고유층까지 침범한 식도암을 내시경 절제술의 절대 적응증으로 제시하였다[1]. 따라서 식도암의 내시경 절제술 전, 내시경, 초음파내시경, 협대역영상(narrow band imaging, NBI) 확대내시경을 이용하여 종양의 심달도를 정확히 평가해야 한다[24-28]. 하지만 시술 전 심달도 평가가 완벽하지는 못하므로 식도절제술의 높은 이환율 및 사망률을 감안할 때 불필요한 수술을 피할 수 있도록 명확한 점막하층 침범이 없는 경우 내시경 절제술을 일차로 시행하는 것이 좋겠다[29-31]. 최근 발표된 국내 연구 결과에 따르면 명확한 점막하층 침범이 없는 표재성 식도편평상피암 환자에서 첫 치료로 내시경 절제술을 받은 군과 식도절제술을 받은 군 간의 장기 생존율의 차이는 없고 치료 후 합병증 발생이 수술을 받은 군 에서 유의하게 높았다[32]. 이는 내시경 절제술 후 불완전 절제(non-curative resection)가 되었던 경우에 추가 수술을 통하여 재발의 위험을 조절할 수 있었기 때문으로 생각된다. 중국의 연구에서도 표재성 식도편평상피암 환자가 내시경 절제술을 받았을 때 수술과 비교하여 생존율의 차이가 없었고 치료 관련 합병증 발생은 더 적었다고 보고되었다[33]. 이러한 결과들을 종합해볼 때 뚜렷한 점막하층 침범 소견이 없는 표재성 식도편평상피암은 수술에 앞서 내시경 절제술을 시행하는 치료 전략이 효과적일 것으로 보인다.
2. 권고안 E2: 표재성 식도편평상피암의 내시경 절제 전 병변의 절제 범위를 결정하기 위하여 루골 색소내시경이나 영상강화내시경 시행을 권고한다(권고등급: 강함, 근거수준: 중등도).
Statement E2: We recommend Lugol chromoendoscopy and/or image-enhanced endoscopy to define the extent of lesion before endoscopic treatment of SESCC (Grade of recommendation: strong, Level of evidence: moderate).
표재성 식도편평상피암은 발적, 미세한 색조 변화나 결절 등의 형태로 발견되고, 다양한 크기의 동시성 병변이 존재하기 때문에 백색광내시경 검사만으로 비암성 병변들과의 감별이 어렵고 병변의 범위, 즉 수평 경계를 정확히 파악하기도 어렵다. 여러 가지 색소내시경 방법 중 루골 용액(Lugol solution)을 이용한 방법이 감별진단을 위하여 가장 효과적이다. 루골 용액을 이용한 색소내시경은 표재성 식도편평상피암 점막 내 케라틴층이 파괴되어 있는 현상을 이용한 것으로, 루골 용액을 병변에 분무하였을 때 정상 점막은 짙은 갈색으로 변하나 표재성 식도편평상피암은 변색하지 않고 옅은 황색으로 남으며, 2~3분 후에 병변의 색깔이 분홍색으로 변화되는 특징적인 pink-color 현상(pink-color sign)을 보인다[34]. 백색광내시경에서 표재성 식도편평상피암으로 의심되는 병변들에 대하여 루골 색소내시경 방법의 유용성을 평가한 연구들에서 고등급 선종 이상의 전암성 병변이나 조기식도암 병변들을 저등급 선종이나 비암성 병변들과 구별하는데 73.8~93.4%의 정확도를 보고하였다[34,35]. 따라서, 이러한 방법은 시술 전 절제 병변의 범위, 수평 경계를 명확하게 구별하는 데 효과적이다.
영상강화내시경은 루골 용액을 이용한 색소내시경에 비하여 병변에 염증 반응을 일으키지 않으며 짧은 시간 내에 관찰할 수 있다는 장점이 있으며, 이 중 협대역영상(NBI)을 이용한 방법이 가장 많이 연구되었다[36]. 90명의 고등급 선종과 표재성 식도편평상피암 환자들을 대상으로 백색광내시경, 루골 색소내시경과 협대역영상의 진단율을 비교한 연구에서 협대역영상을 이용한 내시경 검사의 진단 정확도는 92%로 백색광내시경의 67.8%에 비하여 유의하게 높았으며, 루골 색소내시경의 93.4%와 비슷한 수준이었다[37]. 303명의 표재성 식도편평상피암 고위험군 환자들을 대상으로 루골 색소내시경과 협대역영상내시경의 표재성 식도편평상피암 진단율을 비교한 전향적 연구에서도 협대역영상내시경은 91.2%의 진단 정확도를 보여 루골 색소내시경에 비하여 열등하지 않았다[38]. 이러한 결과들을 고려할 때, 표재성 식도편평상피암의 내시경 절제 전 병변의 절제 범위를 결정하기 위하여 적극적인 루골 색소내시경이나 영상강화내시경 시행을 권고한다.
3. 권고안 E3: 표재성 식도편평상피암의 내시경 절제 전 병기 설정을 위하여 초음파내시경 시행을 권고한다(권고등급: 강함, 근거수준: 중등도).
Statement E3: We recommend endoscopic ultrasound to define the stage of SESCC before endoscopic treatment (Grade of recommendation: strong, Level of evidence: moderate).
식도암의 내시경 치료 후 예후는 병변의 침윤 정도가 얕을수록 좋으며, 위암과 달리 점막근판을 침범한 경우에도 림프절 전이의 위험도가 있다[39]. 그러므로, 식도암의 내시경 치료 전 식도암의 정확한 병기 설정은 매우 중요하다. 표재성 식도편평상피암인 경우 원발암의 침윤 정도(T 병기)와 림프절 전이 여부(N 병기) 판단이 중요하며, 초음파내시경은 침윤 정도와 림프절 전이 여부를 판단하는데 가장 정확한 검사법 중 하나이다. 초음파 내시경을 이용한 식도암의 병기 설정 연구에서 점막층과 점막하층을 침범한 식도암(T1)을 진단하는데 민감도 81.6%, 특이도 99.4%를 보였다[40]. 19건의 관련 논문에 대한 메타분석 연구에서 초음파내시경은 점막층 침범과 점막하층 침범을 감별하는데 좋은 검사법으로 보고되었다(area under the summary ROC curve=0.93) [26]. 또한, 초음파내시경이 식도암의 점막고유층, 점막근판, 점막하층 침윤을 구분할 수 있는지 살펴본 메타분석 연구에서도 초음파내시경의 진단 성적은 우수한 것으로 확인되었다(area under the summary ROC curve=0.98) [11].
4. 권고안 E4: 표재성 식도편평상피암의 내시경 절제 전 협대역영상 확대내시경 검사는 병변의 침윤 깊이 평가에 도움이 된다(권고등급: 약함, 근거수준: 낮음).
Statement E4: We suggest magnifying endoscopy with narrow band imaging for SESCC to assess the depth of invasion before endoscopic treatment (Grade of recommendation: weak, Level of evidence: low).
협대역영상 확대내시경이 식도암의 병변 침윤 깊이를 감별할 수 있는지를 알아본 대규모 다기관 전향 연구에서 편평세포암인 경우 협대역영상 확대내시경은 기존의 내시경보다 우수하지 않다고 보고되었다(협대역영상 확대내시경 정확도 65.3%, 일반내시경 정확도 71.4%, P=0.375) [10]. 일본에서 진행된 다른 전향적 연구에서도 협대역영상 확대내시경이 고해상도 내시경과 고주파 초음파내시경보다 우수하지 않다고 보고되었다[41]. 그러나 최근 발표된 대규모 후향 연구에서 협대역영상 확대내시경은 표재성 식도편평상피암인 경우, 상피층/점막고유층 침윤 진단 양성 예측도가 93%, 점막근판/얕은 점막하층 침윤 진단 양측 예측도가 65%, 깊은 점막하층 침윤 진단 양성 예측도가 77%로 보고되어 표재성 식도편평상피암의 내시경 치료 전 협대역영상 확대내시경이 병변의 침윤 깊이 평가에 도움되는 것으로 보고되었다[42]. 따라서, 시술자의 경험이 풍부한 경우에는 표재성 식도편평상피암 내시경 절제 전 병변의 침윤 깊이 판단을 위하여 협대역영상 확대내시경 검사를 시행하는 것이 유용할 수 있다.
5. 권고안 E5: 점막에 국한된 표재성 식도편평상피암의 내시경 절제술 방법으로 병변의 일괄 절제와 완전 절제를 위하여 내시경 점막 절제술보다는 내시경 점막하 박리술을 시행할 것을 권고한다(권고등급: 강함, 근거수준: 중등도).
Statement E5: We recommend endoscopic submucosal dissection rather than endoscopic mucosal resection for en bloc and curative resection of SESCC confined to the mucosa (Grade of recommendation: strong, Level of evidence: moderate).
내시경 점막 절제술은 상대적으로 시술이 쉽고 합병증의 비율이 낮아 최근까지 널리 사용되어 왔다. 하지만 크기가 큰 병변의 경우 점막 절제술로 일괄 절제가 어려워 2.8~9.8%의 높은 국소 재발이 보고되었다[43-47]. 반면 내시경 점막하 박리술은 시술의 난이도가 높고, 합병증의 위험이 높지만 일괄 절제와 완전 절제율이 높고, 국소 재발률이 낮아 표재성 식도편평상피암 치료에 적합한 방법이다. 시술 방법은 주로 병변의 크기에 따라 결정되고 환자의 전신 상태, 시술자의 경험 등에 따라 선택될 수 있다.
표재성 식도편평상피암 치료에서 내시경 점막 절제술과 내시경 점막하 박리술을 비교한 무작위 배정 연구는 없다. 후향적 연구를 대상으로 한 메타분석에서 병변의 크기와 관계없이 내시경 점막하 박리술군에서 일괄 절제율과 완전 절제율이 높았다. 시술 후 국소 재발률은 내시경 점막하 박리술군에서 0.3%, 내시경 점막 절제술군에서 11.5%로, 내시경 점막하 박리술군에서 유의하게 낮았다(OR=0.08, 95% CI: 0.03~0.23; P<0.001). 시술 후 천공은 내시경 점막하 박리술군에서 유의하게 높았고 (4.0% vs. 1.3%, OR=2.19, 95% CI: 1.08~4.47; P=0.03), 협착, 출혈은 두 군 간에 차이가 없었다[48]. 투명캡을 이용한 내시경 점막 절제술(cap-assisted endoscopic mucosal resection)은 병변의 크기가 10~15 mm 미만인 경우 내시경 점막하 박리술과 비교하여 일괄 절제율, 완전 절제율에 차이가 없다는 보고가 있으나[43,46,47], 다른 메타분석에서는 병변의 크기가 10 mm 미만인 경우에도 내시경 점막하 박리술군에서 일괄 절제율이 더 높았다(OR=3.58, 95% CI: 1.84~7.02; P<0.001) [49].
점막에 국한된 표재성 식도편평상피암 치료에서 내시경 점막하 박리술은 내시경 점막 절제술에 비하여 일괄 절제율 및 완전 절제율이 높고 합병증 위험성은 받아들일 수 있는 수준이므로, 병변의 크기와 관계없이 내시경 점막하 박리술을 먼저 고려할 것을 권고한다. 시술자가 내시경 점막하 박리술의 경험이 많지 않은 경우 크기가 작은 병변에 한하여 선택적으로 내시경 점막 절제술을 고려할 수 있다.
6. 권고안 E6: 식도 내시경 점막하 박리술 후 식도 내강 둘레의 75% 이상에서 점막 결손이 발생한 환자에게 식도 협착을 예방하기 위하여 스테로이드 경구 투약 혹은 스테로이드 국소 주사를 권고한다(권고등급: 강함, 근거수준: 중등도).
Statement E6: We recommend oral steroid or local steroid injection therapy for patients who develop mucosal defects in >75% of the esophageal circumference after endoscopic submucosal dissection to prevent esophageal stricture (Grade of recommendation: strong, Level of evidence: moderate).
식도 내시경 점막하 박리술 후에는 시술 부위에 반흔이 생기면서 식도 협착이 발생할 수 있다. Ono 등[50]의 연구에 따르면, 식도 내강 둘레의 75% 이상에서 점막 결손이 발생한 경우 식도 협착의 위험이 증가한다. 식도 내시경 점막하 박리술 후 내강 둘레의 75% 이상에서 점막 결손이 발생한 환자에서 별도의 처치를 시행하지 않은 경우 66~88%에서 식도 협착이 발생하였다[51-56]. 특히, 내강 둘레의 100%에서 점막 결손이 발생한 환자에서는 식도 협착 치료를 위하여 평균 33.5회의 내시경 풍선 확장술 시술이 필요하였다[57].
식도 내시경 점막하 박리술 후 발생하는 식도 협착을 예방하기 위한 방법으로 스테로이드 경구 투약 혹은 국소 주사 요법이 있다. 스테로이드 경구 투약의 경우, 시술 다음날 혹은 시술 후 이틀 뒤부터 프레드니솔론(prednisolone)을 하루 30 mg 투약하며 2주 내지 12주에 걸쳐 점차 감량 투약한다[54,55,57]. 내시경 점막하 박리술 후 스테로이드를 경구 투약한 환자와 그렇지 않은 환자를 비교한 6개 연구에서 식도 협착 발생 비율은 스테로이드를 투약하지 않은 군에서 69~80%, 스테로이드를 경구 투약한 군에서 18~23%로 스테로이드를 경구 투약할 경우 식도 협착 비율이 73% 가량 유의하게 감소하였다(OR=0.27, 95% CI: 0.13~0.58) [54,55]. 스테로이드 국소 주사도 식도 협착 예방에 효과적이다. 트리암시놀론(triamcinolone)이나 덱사메사손(dexamethasone)을 내시경 점막하 박리술 시행 부위에 국소 주입하였을 때, 식도 협착이 78% 정도 유의하게 감소하였다고 보고되었다(OR=0.32, 95% CI: 0.13~0.83) [51-53,58].
스테로이드 경구 투약과 예방적 내시경 풍선확장술의 효과를 비교하였던 연구에서는 내시경 풍선확장술을 1주에 2회, 총 8주 시행하더라도 32%에서 식도 협착이 발생한 반면, 시술 후 이틀째부터 프레드니솔론 30 mg을 투약하기 시작하여 8주에 걸쳐 감량한 경우에는 식도 협착이 5%에서만 발생하여, 예방적 내시경 풍선확장술보다 스테로이드 경구 투약이 식도 협착 예방 면에서 우월한 효과를 보였다[56].
식도 협착 예방을 위한 스테로이드 투약에 관한 연구는 대부분 협착의 고위험군인 내강 둘레의 75% 이상 점막 결손이 발생한 환자를 대상으로 시행되었다. 한편, 점막 결손의 범위와 상관없이 식도 내시경 점막하 박리술을 시행한 모든 환자를 대상으로 스테로이드 국소 주사의 효과를 살펴본 연구에서도 스테로이드 국소 주사를 시행하지 않은 경우 식도 협착이 36%에서 발생한 반면, 스테로이드 국소 주사 시 식도 협착 발생 비율은 11%로 감소하여 역시 70%의 식도 협착 예방 효과가 있었다(OR=0.30, 95% CI: 0.13~0.83) [58]. 그러나 스테로이드 국소 주사에 따른 식도 천공의 위험성이나 스테로이드 투약 관련 이상 반응 가능성 등을 감안할 때, 스테로이드 경구 투약 혹은 국소 주사 요법은 식도 협착의 고위험군인 내강 둘레의 75% 이상에서 점막 결손이 발생한 환자에 대하여 우선적으로 고려하는 것이 바람직하다.
7. 권고안 E7: 내시경 절제술로 일괄 완전 절제된 표재성 식도편평상피암의 병리조직학적 검사 결과 침윤 깊이가 점막고유층을 넘지 않고 림프관 및 정맥 등 맥관에 암세포 침윤이 없다면 림프절 전이 위험이 매우 낮아서 추가 치료는 필요 없다(권고등급: 강함, 근거수준: 중등도). 점막근판을 침범한 점막암의 경우에도 맥관에 암세포 침윤이 없다면 림프절 전이 위험이 낮아 추가 치료 없이 면밀한 경과 관찰을 고려할 수 있다(권고등급: 약함, 근거수준: 낮음). 점막근판을 넘어서는 침윤, 맥관 암세포 침윤 또는 수직 절제면 침범 양성인 경우는 추가 치료를 권고한다(권고등급: 강함, 근거수 준: 중등도).
Statement E7: No additional treatment is recommended after en bloc complete resection of SESCC invading no more than the lamina propria with no lymphovascular invasion because of a very low risk of lymph node metastasis (Grade of recommendation: strong, Level of evidence: moderate). As the risk of lymph node metastasis of a tumor invading into the muscularis mucosa without lymphovascular invasion is low, a close follow-up after en bloc complete endoscopic resection can be considered without additional treatment (Grade of recommendation: weak, Level of evidence: low). In case of a tumor with submucosal invasion, lymphovascular invasion, and/or positive vertical resection margin, additional treatment is recommended (Grade of recommendation: strong, Level of evidence: moderate).
표재성 식도편평상피암의 림프절 전이 위험성은 종양의 심달도와 밀접한 관계가 있으므로 내시경 절제술 후 완치를 기대할 수 있는 완전 절제(curative resection) 여부를 평가할 때 심달도가 매우 중요하다[59-61]. 식도암으로 식도절제술 및 주변림프절 곽청술을 받은 환자들의 병리조직을 분석한 결과에 따르면 식도암이 점막하층으로 침윤하면 26.0~53.8%의 림프절 전이 위험성이 있다[59-68]. 점막하층 상부 1/3까지만 침범한 경우로 국한하였을 때도 8.3~53.1%에서 림프절 전이가 확인되었다. 한편, 일본 식도암 연구회와 유럽내시경학회 가이드라인에서는 점막 근판으로부터 200 μm 이하의 얕은 점막하층 침윤을 보이는 표재성 식도편평상피암을 내시경 절제술의 상대 적응증에 포함시키고 있는데, 이와 같이 200 μm 이하의 얕은 점막하층 침윤을 보이는 표재성 식도편평상피암의 림프절 전이 빈도에 대한 자료는 매우 제한적이다[67]. 식도암이 점막층에 국한된 경우 림프절 전이 빈도는 0~15.4%로 점막하층을 침범한 식도암에 비하여 낮지만 무시할 수 있는 수준은 아니다[59-67]. 이들을 다시 점막고유층까지 국한된 경우와 점막근판까지 침범한 경우로 나누어 림프절 전이 빈도를 보면 각각 0~8.7% 및 8~27%로 점막근판까지 침범한 경우 림프절 전이 위험도가 뚜렷하게 높다. 림프절 전이 위험은 암세포의 림프관 또는 정맥 등 맥관 침윤과도 관련성이 있다[59,65,67,69,70]. 일본의 한 대규모 연구에 따르면, 점막근판을 침범한 식도암에서 내시경 절제술 후 림프관 침윤이 없는 것으로 확인된 경우 5년 누적 원격 전이 발생률은 0.7%로 매우 낮아 점막근판까지 침범한 표재성 식도편평상피암이라 하더라도 맥관에 암세포 침윤이 없다면 내시경 절제술 적응증이 될 수 있음을 시사하였다[68]. 국내 두 기관에서 보고한 내시경 절제술 치료 성적에서도 점막층까지를 완전 절제(curative resection) 심달도 기준으로 하였을 때 완전 절제된 환자들의 장기 추적 도중 식도암으로 인한 사망은 없어서 점막층까지가 내시경 절제술의 안전하고 효과적인 심달도 기준이 될 수 있다는 주장의 근거가 된다[71,72]. 일부 보고에서는 식도암의 미분화형이 림프절 전이 위험성과 연관 있다고 하였지만[65], 그렇지 않은 결과를 보여주는 연구들도 많아 미분화형 식도암을 내시경 절제술 후 불완전 절제(non-curative resection)의 기준으로 확정할 수는 없으며, 명확한 결론을 위하여 향후 추가적인 자료 분석이 필요하다[59,61,68]. 종합하면, 내시경 절제술로 일괄 완전 절제된 표재성 식도편평상피암의 병리조직학적 검사 결과 침윤 깊이가 점막고유층까지이고 림프관이나 정맥 등 맥관에 암세포 침윤이 없다면 완치를 기대할 수 있는 완전 절제(curative resection)로 판단하고 추가 수술 없이 경과 관찰할 수 있다. 점막근판까지 침윤한 표재성 식도편평상피암이고 맥관 암세포 침윤이 없는 경우에도 림프절 전이 위험도가 높지 않으므로 내시경 절제술로 일괄 완전 절제되었다면 환자의 연령, 동반 질환, 전신 상태 등 수술의 위험도를 고려한 후 추가 수술 없이 경과 관찰을 고려할 수 있다. 만약, 일괄 절제되지 못하였다면 병리 조직학적 평가가 불충분하였을 수 있음을 감안한 추적 관찰 전략이 필요하다.
내시경 절제술 검체에 대한 병리 검토 결과 암세포의 점막하층 침윤, 맥관 침윤 또는 수직 절제면 침범 양성 소견 등이 발견되어 림프절 전이 가능성이 있고 이로 인하여 불완전 절제로 판단되는 경우에는 추가 치료가 필요하며, 식도절제술 및 주변 림프절곽청술이 표준 치료법이다. 그러나 식도절제술은 수술 후 30~40%의 높은 이환율과 최소 1~2%의 사망률을 동반하므로 환자의 전신 상태 등을 모두 고려하여 시행 여부를 결정해야 한다[29-31]. 표재성 식도편평상피암에 대한 내시경 절제술 후 불완전 절제로 판정된 경우에 대하여 방사선 항암 치료를 시행한 연구들이 비교적 양호한 치료 성적을 보고하고 있어 방사선 항암 치료가 향후 새로운 추가 치료 전략으로 자리잡을 가능성도 있을 것으로 기대된다[73-78].
조기위암
1. 권고안 G1: 조기위암의 내시경 절제 전 병변의 절제 범위를 결정하기 위하여 색소내시경이나 영상강화내시경 시행을 권고한다(권고등급: 강함, 근거수준: 중등도).
Statement G1: We recommend chromoendoscopy/image-enhanced endoscopy to determine the extent of lesion before endoscopic treatment of early gastric cancer (Grade of recommendation: strong, Level of evidence: moderate).
내시경 절제술 전 병변의 수평 경계를 명확히 파악하는 것은 국소 재발을 줄이고 완치율을 높이는 데 매우 중요하다. 병소의 경계를 평가하기 위하여 전통적으로 색소내시경이 널리 사용되었으며, 최근 내시경 기술의 발달로 인하여 협대역영상(NBI) 및 확대내시경 등 다양한 방법의 영상강화내시경이 임상에서 많이 이용되고 있다[12,79]. 인디고카민(indigocarmine)을 이용한 색소내시경으로 조기위암의 경계를 관찰하였을 때 일반 백색광내시경에 비하여 경계 예측의 정확도가 더 높았고(75.9% vs. 50.0%), 인디고카민과 아세트산을 같이 투여한 색소내시경의 경우 병변의 경계를 90.7%까지 정확히 예측한다고 보고하였다[80]. 국내 연구 결과 또한 인디고카민과 아세트산을 같이 투여하여 색소내시경을 시행한 경우 일반 백색광내시경에 비하여 조기위암의 경계를 더 정확히 예측할 수 있었다(84.1% vs. 66.9%)[81]. 또한, 조기위암의 경계 평가를 위하여 협대역영상 확대내시경과 인디고카민 색소내시경을 비교한 연구에서는 협대역영상 확대내시경이 인디고카민 색소내시경에 비하여 보다 정확히 수평 경계를 예측할 수 있었다(81.1% vs. 72.6%) [12]. 협대역영상 확대내시경은 일반 백색광내시경과의 비교에서도 병변 경계를 관찰하는데 민감도와 특이도 모두 우월하였다(민감도 92.9% vs. 42.9%, 특이도 94.7% vs. 61.0%) [13]. 이러한 결과들을 고려할 때, 조기위암의 내시경 절제 전 병변의 절제 범위를 결정하기 위하여 적극적인 색소내시경이나 영상강화내시경 시행을 권고한다.
2. 권고안 G2: 조기위암의 내시경 절제술 전 내시경초음파는 일부 환자에서 침윤 깊이 평가에 도움이 된다(권고등급: 약함, 근거수준: 중등도).
Statement G2: Endoscopic ultrasonography before endoscopic resection of early gastric cancer may be helpful in determining the depth of invasion in some patients with early gastric cancer (Grade of recommendation: weak, Level of evidence: moderate).
내시경초음파는 위암의 침윤 깊이와 국소 림프절 전이 여부 평가를 위하여 유용하게 사용될 수 있다. 5,601명의 위암 환자를 대상으로 원발암 침윤도, 즉 T 병기를 예측하는데 있어 내시경초음파의 유용성을 평가한 54개 연구를 메타분석한 보고에 의하면, 내시경초음파는 T3~4 병변과 T1~2 병변을 구분하는데 있어 민감도 86%, 특이도 91%로 정확하였다[14]. 하지만 조기 위암에서 내시경 절제술 전 내시경초음파 소견으로 조기위암의 침윤 깊이를 정확히 예측하는 것은 제한이 있다[82-88]. 국내 대규모 전향적 연구에 의하면, 조기위암에서 점막층과 점막하층 침범을 구분하는데 있어 정확도는 내시경초음파가 67.4%로 일반내시경의 73.7%에 비하여 우월하지 않았다[84]. 국내에서 시행된 다른 연구에서도 조기위암의 침윤 깊이 예측 정확도에 있어 미세탐촉자를 이용한 초음파내시경은 백색광내시경에 비하여 통계적으로 유의한 차이가 없었다(81.4% vs. 78.9%) [83]. 그러나 일부 연구에서는 내시경초음파가 조기위암의 침윤 깊이를 파악하는데 있어 도움을 줄 수 있다고 보고하고 있다. 국외에서 시행한 한 연구에 따르면, 조기위암 침윤 깊이 예측에 있어 내시경초음파의 진단 정확도가 백색광내시경보다 더 높았다(71% vs. 63%) [85]. 최근 발표된 다른 연구에서는 조기위암의 침윤 깊이를 예측하는데 있어 색소내시경에 비하여 내시경초음파의 정확도가 더 높았고(79.1% vs. 76.5%), 색소내시경과 내시경초음파를 함께 시행하였을 경우 침윤 깊이를 88.3%까지 정확히 예측할 수 있었다[82]. 따라서, 조기위암의 점막층 또는 점막하층 침윤 감별에 있어 내시경초음파는 도움이 될 가능성이 있는데, 특히 내시경 육안 소견에서 점막하층을 침범한 소견이 의심되는 경우 등 일부 환자에서 내시경 절제술 전 병변의 침윤 깊이를 보다 세밀하게 평가하는 데에 유용할 것으로 생각된다[89].
3. 권고안 G3: 분화형 선암(well or moderately differentiated tubular or papillary adenocarcinoma)이고 궤양이 없으면서 내시경 소견으로 점막하 침윤이 의심되지 않는 직경 2 cm 이하의 육안적 점막 침범 조기위암은 내시경 절제술을 권고한다(권고등급: 강함, 근거수준: 중등도).
Statement G3: We recommend endoscopic resection for early gastric cancer of well or moderately differentiated tubular or papillary adenocarcinoma meeting endoscopically estimated tumor size ≤2 cm and endoscopically suspected mucosal cancer without ulcer (Grade of recommendation: strong, Level of evidence: moderate).
내시경 절제술은 림프절 전이 위험도가 거의 없는 조기위암에서 시행할 수 있는 국소 치료이다. 2000년 Gotoda 등[90]에 의하여 확대 적응증이 제안되기 이전까지는 분화형 선암(well or moderately differentiated tubular or papillary adenocarcinoma)이고 궤양이 없으면서 점막하 침윤이 의심되지 않는 직경 2 cm 이하의 점막층에 국한된 조기위암이 내시경 절제술의 적응증으로 받아들여졌으며, 따라서 이들에 대해서는 내시경 절제술을 첫 치료로 고려해야 한다. 조기위암의 내시경 절제를 고려함에 있어서 가장 중요한 인자는 림프절 전이 위험도인데, 상기 적응증을 만족하는 병변에서는 림프절 전이 위험도가 무시할 정도로 매우 낮음이 여러 연구들에서 보고되었다(0~0.3%) [90-92]. 또한, 내시경 절제술 후 장기 생존율을 수술 후 장기 생존율과 비교 분석한 결과도 보고되었는데, 국내 여러 연구들에서 내시경 절제술 후 5년 생존율은 93.6~96.4%로 수술 후 5년 생존율인 94.2~97.2%와 차이가 없었고[93-95], 10년 생존율 또한 내시경 절제술 후 81.9%, 수술 후 84.9%로 의미있는 차이를 보이지 않았다[93]. 하지만 5년 누적 이시성 위암 재발률은 수술과 비교하였을 때 내시경 절제술을 시행한 경우가 의미있게 높았다(0.9~1.1% vs. 5.8~10.9%) [93-95]. 내시경 절제술의 경우 위 전체를 보존하기 때문에 수술과 비교하였을 때 잔존 위에서의 이시성 위암 재발률이 높을 것으로 생각된다. 따라서, 내시경 절제술로 완전 절제된 후에도 이시성 위암 재발을 감시하기 위한 지속적 내시경 추적검사가 필요하다. 한편, 내시경 절제술은 위 전체를 보존함으로써 수술에 비하여 삶의 질이 향상되고, 시술과 관련된 합병증이 적으며, 입원 기간이나 비용 측면에서 경제적이다[93-98]. 결론적으로, 분화형 선암(well or moderately differentiated tubular or papillary adenocarcinoma)이고 궤양이 없으면서 내시경 소견으로 점막하 침윤이 의심되지 않는 직경 2 cm 이하의 육안 소견상 점막 침범 조기위암에서는 수술과 동등한 종양학적 생존율, 양호한 삶의 질, 경제적 관점에서의 우수성 등을 고려할 때 내시경 절제술이 우선적인 치료법으로 권고된다[93-96].
4. 권고안 G4: 분화형 선암(well or moderately differentiated tubular or papillary adenocarcinoma)이면서 내시경 소견에서 1) 궤양이 없고 크기가 2 cm를 초과하는 점막암이거나, 2) 궤양이 있으면서 크기가 3 cm 이하인 점막암의 경우 내시경 절제술 시행을 권고한다 (권고등급: 약함, 근거수준: 중등도).
Statement G4: We suggest endoscopic resection for early gastric cancer of well or moderately differentiated tubular or papillary adenocarcinoma meeting the following endoscopic findings: 1) mucosal cancer >2 cm without ulcer, or 2) mucosal cancer ≤3 cm with ulcer (Grade of recommendation: weak, Level of evidence: moderate).
표준적인 위암의 조직형 분류는 2000년 세계보건기구(World Health Organization, WHO) 분류법을 따르며, WHO 분류법에서의 미분화암(undifferentiated carcinoma)은 선구조나 편평상피 등으로의 분화가 없는 경우로 한정하고 있다. 그러나 다수의 내시경 절제술 관련 연구들에서는 고분화 및 중등도 분화 관상선암(well differentiated tubular adenocarcinoma, moderately differentiated tubular adenocarcinoma) 또는 유두상 선암(papillary adenocarcinoma)을 분화형 선암(differentiated type adenocarcinoma)으로 분류하며, 저분화 관상선암(poorly differentiated tubular adenocarcinoma) 또는 약응집암(poorly cohesive carcinoma)을 미분화형 선암(undifferentiated type adenocarcinoma)으로 간주하고 있다. 내시경 절제술 적응증의 확대는 기존의 표준 치료인 수술과 비교하였을 때 생존율 차이가 없는 경우에 고려되어야 한다. 또한, 어느정도의 림프절 및 원격 전이 위험도를 허용 가능한 수준으로 볼 것인지는 수술 사망률과의 비교, 검토를 통하여 판단해야 한다. 일반적으로 림프절 및 원격 전이 위험도는 종양의 크기, 분화도, 종양의 침범 깊이 및 림프관이나 정맥관 같은 맥관 침윤 여부 등을 통하여 검토, 추정된다. 분화형 선암(well or moderately differentiated tubular or papillary adenocarcinoma) 이고 내시경 소견에서 궤양이 없고 크기가 2 cm를 초과하는 조기위암이나, 궤양이 있으면서 크기가 3 cm 이하인 조기위암이면서 내시경 절제술 후 병리조직 검사에서 맥관 침윤이 없고 절제면이 음성인 점막암인 경우, 림프절 및 원격 전이 가능성은 0~0.21%로 보고되어 위절제술 후 사망률인 0.1~0.3%와 비교하여 차이가 없으므로 내시경 절제술을 시행할 수 있는 근거가 될 수 있다[99-101]. 또한, 수술적 절제와 내시경 절제술의 생존율을 비교한 연구에서도 5년 생존율이 각각 92.0~97.2%와 93.3~96.4%로 유의미한 차이가 없어, 이러한 병변에서는 완전 절제(curative resection)로 판단하여 위절제술 등의 추가 치료가 필요하지 않다[95,100,102-109].
시술 전 평가에서 점막하층 침윤이 의심될 경우 표준 치료는 수술적 절제이다. 하지만 수술 전 평가에서 점막하층 침윤이 의심되어 위절제술을 시행받은 환자의 최종 병리 결과를 분석한 연구들에서 28.8~43%의 병변이 내시경 절제술로 완전 절제(curative resection)될 수 있었던 것으로 보고되고 있어, 수술 전 평가에서 점막하층 침윤이 의심되는 경우의 치료 방침에 대해서는 추가 연구가 필요할 것으로 생각된다[110,111].
5. 권고안 G5: 미분화형 선암(poorly differentiated tubular adenocarcinoma, poorly cohesive carcinoma, and signet ring cell carcinoma)이고 내시경 소견에서 궤양이 없고, 크기가 2 cm 이하인 점막층에 국한된 조기위암은 내시경 절제술 시행을 권고한다(권 고등급: 약함, 근거수준: 낮음).
Statement G5: We suggest endoscopic resection for poorly differentiated tubular adenocarcinoma, poorly cohesive carcinoma, and signet ring cell carcinoma meeting the following endoscopic findings: endoscopically estimated tumor size ≤ 2 cm, endoscopically mucosal cancer, and no ulcer in the tumor (Grade of recommendation: weak, Level of evidence: low).
저분화 관상선암(poorly differentiated tubular adenocarcinoma), 약응집암(poorly cohesive carcinoma) 및 반지세포암(signet ring cell carcinoma)을 포함하는 미분화형 선암(undifferentiated type adenocarcinoma)의 경우 림프절 전이 빈도가 높다는 여러 연구들로 인하여 미분화형 조기위암은 내시경 절제술의 전통적인 적응증으로 인정되지 못하였다[112,113]. 그러나 크기가 2 cm 이하이면서 점막에만 국한된 미분화형 선암인 조기위암에 대하여 내시경 절제술을 시행받은 환자들을 대상으로 한 후향적 연구들에서 이러한 경우에 림프절 및 원격 전이의 빈도가 극히 낮으며 5년 생존율은 95~98.6%로 보고하였다[100,114-118]. 또한, 내시경 절제술을 시행한 군과 수술적 절제를 받은 군의 장기 성적을 비교한 연구들에서도 유의한 차이가 없는 것으로 보고하여 이러한 경우 수술적 절제뿐 아니라 내시경 절제술도 권고할 수 있다[95,100,103,118]. 그러나 미분화형 선암은 경계가 불확실한 형태가 많아 완전 절제율이 45.1~70%로 낮다는 국내 보고가 있어, 경계 확인에 주의를 요하며 내시경 절제술 시행 시 충분한 절제연의 확보가 필요하다[115,116]. 또한 미분화형 선암인 조기위암 내에서도 저분화 관상선암과 약응집암 및 반지세포암은 생물학적 행태가 다를 수 있어 향후 이러한 부분에 대한 추가적 연구가 필요하다.
6. 권고안 G6: 내시경 절제술 직후 절제 궤양면에서 관찰되는 혈관들을 사전 지혈하는 것이 지연성 출혈의 발생을 감소시킨다(권고등급: 강함, 근거수준: 낮음).
Statement G6: We recommend prophylactic hemostasis of visible vessels on the postresection ulcer caused by endoscopic resection of early gastric cancer to lower the risk of delayed bleeding (Grade of recommendation: strong, Level of evidence: low).
7. 권고안 G7: 내시경 절제술 시 양성자펌프억제제 사용은 의인성 궤양으로 인한 증상과 합병증을 감소시킨다(권 고등급: 강함, 근거수준: 높음).
Statement G7: We recommend proton pump inhibitors to decrease the risk of symptoms and complications associated with iatrogenic ulcers caused by endoscopic resection of early gastric cancer (Grade of recommendation: strong, Level of evidence: high).
내시경 절제술 관련 출혈은 정의에 따라 그 빈도가 다양하게 보고되고 있는데, 시술 도중 수혈이 요구되거나 외과적 수술이 필요한 심각한 즉시 출혈은 1% 미만에서 발생하는 것으로 보고되었다[119]. 내시경 절제술 후에 발생하는 지연 출혈은 지혈술이 필요한 의인성 궤양으로부터의 출혈을 의미하며 1.3~11.9%로 보고되었다. 일반적으로 시술 후 24시간 이내 발생이 가장 흔하지만 시술 후 2주까지 발생할 수 있다[120,121]. 내시경 절제술 후 지연 출혈을 예방하기 위하여 시술 후 의인성 궤양의 바닥에서 관찰되는 노출 혈관을 사전 지혈하는 것은 효과적인 방법이다. 한 후향적 연구에서 사전 지혈을 하지 않으면 지연 출혈의 위험도가 2.47배 증가한다고 보고하였다[122]. 그러나 사전 지혈을 과도하게 할 경우 응고증후군이나 지연 천공 발생 위험성이 높아질 수 있어 주의를 요한다[123,124].
지연 출혈을 예방하기 위하여 시술 후 양성자펌프억제제나 히스타민-2 수용체길항제를 투여하는 것이 도움이 된다. 내시경 절제술과 관련한 의인성 궤양의 치유를 위하여 사용하는 양성자펌프억제제와 히스타민-2 수용체길항제의 효과를 비교한 연구에서는 양성자펌프억제제가 더 효과적이라는 보고도 있지만[125,126] 두 가지 약제의 효과가 유사하다는 결과들도 있어서[127,128] 특정 약제의 우월성은 명확하지 않다. 한 메타분석에서는 의인성 궤양의 지연 치유 여부와 증상 호전에 관하여 양성자펌프억제제와 히스타민-2 수용체길항제의 효과에 차이가 없었지만 양성자펌프억제제군에서 지연 출혈의 빈도는 유의하게 낮은 것으로 나타났다(OR=0.49, 95% CI: 0.25~0.95) [129]. 그 외에 의인성 궤양의 치유 효과를 위한 양성자펌프억제제의 용량, 투약 기간 그리고 점막보호제의 병용 투약에 대해서는 다양한 보고들이 있다[130-142]. 지연 출혈을 예방하기 위하여 내시경 절제술 전에 양성자펌프억제제를 투약하는 방법은 무작위 비교 연구에서 지연 출혈의 감소에 더 효과적이지는 않은 것으로 보고되었으며, 시술 후에 2차 내시경을 시행하는 방법도 지연 출혈 감소에 통계적으로 유의하게 효과적이지는 않았다[143-145].
8. 권고안 G8: 내시경 절제술 중에 천공이 발생하였을 경우 내시경 치료가 1차 치료로 권고된다(권고등급: 강함, 근거수준: 낮음).
Statement G8: We recommend endoscopic closure as the first treatment option for perforation that occurred during endoscopic resection of early gastric cancer (Grade of recommendation: strong, Level of evidence: low).
내시경 절제술 중 고유근층에 대한 과도한 손상으로 발생하는 시술 중 천공의 빈도는 1.2~5.2%이며, 시술 후에 나타나는 지연 천공은 0.5% 이내의 발생률로 보고되고 있다. 이러한 천공은 병소의 크기나 위치에 따라 발생 위험도가 다르다[146]. 시술 도중 천공이 발생하였을 때 일차적으로 내시경클립술을 이용하여 봉합하는 것이 효과적이며, 성공적인 봉합 후에 금식과 항생제 투약의 보존적 치료를 하면 대부분 외과적 치료 없이 호전되었음을 보고하였다[147-149]. 그러나 봉합에 실패하거나 범발성 복막염의 징후를 보일 때 외과적 치료를 고려해야 하며 천공이 늦게 진단된 지연 천공의 경우에도 외과적 치료가 필요할 수 있다[150]. 내시경을 통한 봉합은 숙련된 내시경 의사에 의하여 시행하는 것이 중요하며, 긴장성 공기복강증(tension pneumoperitoneum)이 발생하여 혈역학적 불안정성을 보이거나 호흡 장애가 발생하면 복강 내 공기 흡인/배출을 위한 경피적 천자 및 배액관을 통한 신속한 복강 내 감압이 필요하다[151]. 또한 천공이 발생하였을 때 내시경 도중 공기 대신 이산화탄소 주입으로 변경하는 것이 도움이 될 수 있다[152].
9. 권고안 G9: 조기위암의 내시경 절제술 후 병리조직학적 검사에서 불완전 절제(non-curative resection) 기준에 해당되는 경우 외과적 절제 시행을 권고한다. 단, 수평 절제연만 암세포 침범을 보이는 경우는 예외로 한다(권고등급: 강함, 근거수준: 중등도).
Statement G9: We recommend surgical gastrectomy if histopathological evaluation after endoscopic resection of early gastric cancer meets the criteria for non-curative resection. An exception applies if cancer invasion is observed at the horizontal resection margin only (Grade of recommendation: strong, Level of evidence: moderate).
10. 권고안 G10: 조기위암의 내시경 절제술 후 병리조직학적 검사에서 다른 불완전 절제(non-curative resection) 기준에 해당하지 않으면서 수평 절제연만 암세포 침범을 보이는 경우에는 외과적 절제보다는 추가적 내시경 치료 시행을 권고한다(권고등급: 강함, 근거수준: 중등도).
Statement G10: We recommend additional endoscopic management rather than surgical gastrectomy if histopathological evaluation of endoscopically resected early gastric cancer specimen shows positive involvement at the horizontal resection margin without any other findings compatible with non-curative resection (Grade of recommendation: strong, Level of evidence: moderate).
병소가 내시경 절제로 일괄 절제가 되었으며 절제 후 최종 조직병리 소견에서 림프관 및 정맥 등 맥관 침윤 없이 궤양을 동반하지 않은 점막에 국한된 2 cm 미만의 분화형 선암(well or moderately differentiated tubular or papillary adenocarcinoma)이고 절제연 음성인 경우를 절대 적응증 병소의 완전 절제(curative resection)로 간주한다. 병소가 일괄 절제가 되었으며 맥관 침윤이 없고 절제연 음성인 경우 중 분화형 선암이면서 궤양을 동반하지 않은 2 cm 이상의 점막암, 3 cm 이하의 궤양을 동반한 점막암, 3 cm 이하의 점막하 침윤암이면서 점막하층 침윤 깊이가 500 μm 이하인 경우 또는 2 cm 이하의 미분화형 선암(poorly differentiated tubular adenocarcinoma, poorly cohesive carcinoma, and/or signet ring cell carcinoma)이면서 점막에 국한된 조기위암은 확대 적응증 병소의 완전 절제(curative resection)로 정의한다. 이상의 완전 절제 기준에 해당하지 않는 병소는 불완전 절제(non-curative resection)로 간주한다[1,120,153]. 이 중 수평 절제연 양성만 해당되는 경우를 제외하고 다른 불완전 절제의 기준에 해당하는 경우에서의 림프절 전이 빈도는 분화형 선암인 경우 2.6~3.0%로 보고되고 있고, 미분화형 선암에서는 5~20% 이상에 이르는 것으로 보고되고 있다[90,154,155]. 불완전 절제 기준에 해당하여 추가적인 외과 수술을 시행한 대규모 코호트를 대상으로 림프절 전이 위험도를 분석하였을 때, 림프관 침윤이 가장 높은 위험성 증가를 보였다. 그 외에 종양의 크기가 큰 경우, 수직 절제연(vertical resection margin) 양성인 경우, 맥관 침윤을 보이는 경우 그리고 500 µm를 초과하는 점막하 침윤을 보이는 경우는 유사한 정도의 림프절 전이 위험도 증가를 보이는 것으로 보고하였다[156]. 림프맥관 침윤이 림프절 전이의 중요한 위험인자임은 많은 근거를 통하여 제시되었다[157-159]. 따라서 이러한 림프절 전이의 위험성을 고려한다면, 수평 절제연 양성 이외의 다른 불완전 절제기준에 해당하는 경우에는 주변림프절곽청술을 포함한 추가적인 외과 수술이 필요하다. 다만, 분화형 선암이면서 2 cm 이하의 점막암에서 맥관 침윤이 동반되었을 경우에는 림프절 전이의 위험성이 높지 않다는 보고가 있어서 이에 해당하는 경우에 추가적인 외과 수술의 필요성은 아직 명확하지 않다[160]. 불완전 절제 후 외과적 절제를 시행한 환자군을 추가적인 치료를 하지 않은 환자군과 비교한 일부 연구에서는 추가적인 치료의 이득이 없다는 보고를 하기도 하였지만[161-163], 대부분의 후향적 연구들에서 외과적 절제를 하였을 때 더 높은 전체 생존율과 질병 특이 생존율을 보였으며[158,159,164-167], 특히 고령의 환자들에서도 불완전 내시경 절제 후에 추가적인 외과적 절제를 적극적으로 시행함으로써 생존율 향상에 이득이 있음이 제시되었다[168-170].
일괄 절제가 이루어진 분화형 선암에서 수평 절제연만 양성이면서 다른 완전 절제의 요건을 충족한 경우에 림프절 전이의 위험성은 매우 낮다. 이런 경우에 추가적인 치료 없이 장기 추적한 코호트에서 낮은 5년 재발률을 보였으며 재발의 경우에도 위암 관련 사망 없이 완치적 치료가 가능하였다[171]. 따라서 수평 절제연 양성 환자에서는 외과적 절제를 하지 않고 추가적인 내시경 절제술을 시행하거나 아르곤플라즈마응고술을 사용하여 내시경소작술을 시행할 수 있으며 후향적 코호트 연구들에서 이러한 추가적인 내시경 치료 후 좋은 장기 예후를 제시하였는데, 특히 3개월 이내의 추가적인 내시경 치료가 낮은 재발률과 관련이 있다[172-174]. 그러나 내시경소작술은 최종적인 조직학적 평가가 어렵기 때문에 추가적인 내시경 치료 후의 완전 절제를 평가하는 것이 불가능하여 시술 후 면밀한 추적 관찰이 필요하다.
11. 권고안 G11: 헬리코박터 파일로리에 감염되어 있는 조기위암 환자에서는 내시경 절제술 후 제균 치료가 필요하다(권고등급: 강함, 근거수준: 높음).
Statement G11: We recommend Helicobacter pylori eradication treatment after endoscopic resection of early gastric cancer in Helicobacter pylori -infected patients (Grade of recommendation: strong, Level of evidence: high).
조기위암의 내시경 치료 후 헬리코박터 파일로리 양성인 경우 이시성 재발을 감소시키기 위하여 제균 치료를 고려할 수 있다. 2008년 Fukase 등[175]은 조기위암 환자의 내시경 치료 후 헬리코박터 파일로리 제균 치료로 이시성 위암 발생 위험도를 유의하게 감소시킨다는 다기관 연구 결과를 보고하였다(hazard ratio [HR]=0.339, 95% CI: 0.157~0.729). 이에 근거하여 대부분의 임상진료지침에서 조기위암 환자의 내시경 치료 후 헬리코박터 파일로리 제균 치료를 추천하고 있다[176-180]. 조기위암의 내시경 치료 후에 헬리코박터 파일로리 제균 치료가 이시성 위암을 예방하는가에 관한 4개의 메타분석에서는 제균 치료를 하는 경우 이시성 위암 발생에 대한 위험도를 0.42~0.51로 유의하게 감소시킨다고 보고하였다[181-184]. 국내에서도 위약 대조군 전향적 무작위 배정 연구를 시행하여 2018년에 그 결과가 발표되었는데, 제균 치료군에서 약 50%의 이시성 위암 발생을 예방할 수 있었고, 제균이 실제 성공적으로 이루어진 군에서는 이시성 위암 발생을 약 68%나 줄일 수 있었다[185]. 2018년에 발표된 다른 국내의 전향적 무작위 배정 연구에서는 제균 치료군에 비하여 대조군에서 이시성 위암 발생 위험도가 2.02배 증가하였음을 보여주었다[186]. 따라서, 조기위암의 내시경 치료 후에 이시성 위암 재발 방지를 위하여 헬리코박터 파일로리 제균 치료가 권고된다.
12. 권고안 G12: 조기위암의 이시성 재발을 조기에 발견하기 위하여 절대 적응증 또는 확대 적응증으로 완전 절제(curative resection)된 환자를 대상으로 6~12개월 간격의 정기적 내시경 시행을 권고한다(권고등급: 강함, 근거수준: 낮음).
Statement G12: We recommend regular surveillance endoscopy every 6~12 months for patients who have had curative endoscopic resection of early gastric cancer based on absolute or expanded criteria for early detection of metachronous gastric cancer (Grade of recommendation: strong, Level of evidence: low).
내시경 치료 후 추적검사 계획은 기본적으로 외과적 위절제술을 시행받은 환자와 유사하지만 조기위암의 내시경 절제술 후에는 동시성 다발성 위암 및 이시성 위암의 빈도가 높은 점에 특별히 더 유의하면서 면밀한 추적검사를 해야 한다. 우리나라 위암표준진료권고안에서는 조기위암으로 내시경 치료를 받은 환자에서 매년 내시경 추적검사를 시행하도록 권고하고 있다[187]. 일본의 진료지침에서는 내시경 완전 절제 후에 이시성 위암 발견을 위하여 6~12개월 간격으로 내시경 검사를 시행하며, 확대 적응증에 해당하는 경우 전이 발견을 위하여 내시경 검사와 더불어 초음파 또는 컴퓨터단층촬영술을 6~12개월 간격으로 시행할 것을 권고하고 있다[7,120]. 유럽 진료지침에서는 내시경 완전 절제 후 3~6개월 뒤, 이후에는 1년마다 정기적 내시경 검사를 시행하며, 확대 적응증 병변에서는 복부 컴퓨터단층촬영술을 고려할 수 있다고 하였다[1].
내시경 치료 후 추적검사 목적은 국소 재발, 동시성 및 이시성 위암 발견 그리고 위 밖으로의 전이 발견이다. 내시경 치료 후 국소 재발은 한 메타분석에서 내시경 점막하 박리술군에서 0.3%, 내시경 점막 절제술군에서 5.2%로 보고하였고[49], 2018년 발표된 국내 다기관 전향적 연구에서는 내시경 점막하 박리술 후 완전 절제군에서 0.7%, 불완전 절제군에서 2.4%로 보고하였다[188]. 따라서 완전 절제된 내시경 점막하 박리술의 경우 대부분 1% 미만의 국소 재발률을 보이고 있어 국소 재발보다는 동시성 또는 이시성 위암을 찾는 노력이 중요하다. 내시경 치료를 받은 조기위암 환자는 위점막의 대부분이 그대로 남아 있어 동시성 및 이시성 위암 발생이 수술 환자보다 흔하다. 내시경 치료 시점부터 1년 미만의 시기에 발견된 암을 동시성 위암으로, 1년 이상 경과한 후에 발견된 암을 이시성 위암으로 정의하면 동시성 위암의 발생률은 0.87~11%, 이시성 위암 발생률은 3.6~22.7%로 다양하게 보고되어 있다[101,189-191]. 2015년 보고된 한 일본 연구에서는 내시경 점막하 박리술로 완전 절제한 이후 이시성 재발률이 5년, 7년, 10년에 각각 9.5%, 13.1%, 22.7% 로 증가한다고 보고하였고[191], 또 다른 일본의 다기관 연구에서는 이시성 위암의 연평균 발생률을 3.5%로 보고하였다[189]. 최근 국내에서 시행된 연구에서는 동시성 및 이시성 위암의 연평균 발생률이 2.47%이며, 1년을 초과하여 추적검사를 시행한 경우 1년 이하 기간으로 추적검사를 시행한 군과 비교하여 이시성 위암 발생 시 수술이 필요한 비율이 의미 있게 높았다고 보고하였다[192]. 이러한 결과들을 종합하면, 내시경 치료 후 발생되는 동시성 및 이시성 위암의 조기 발견이 성공적인 추적 진료를 위하여 매우 중요하며, 내시경 치료 후 5년 동안에는 국소 재발, 동시성 및 이시성 위암 발견을 위하여 6~12개월 간격으로 내시경 추적검사가 필요하다. 또한, 치료 5년 이후에도 이시성 위암 발생이 지속적인 증가를 보이기 때문에 5년 이후에도 내시경 추적검사를 시행하는 것이 바람직하다[191,193]. 내시경 추적검사의 간격 및 기한에 대한 보다 자세하고 정확한 기준은 추후 잘 고안된 연구를 통하여 확정할 필요가 있다.
13. 권고안 G13: 위 밖에서의 재발을 발견하기 위하여 절대 적응증 또는 확대 적응증으로 완전 절제(curative resection)된 환자를 대상으로 6~12개월 간격의 정기적인 CT 검사를 권고한다(권고등급: 약함, 근거수준: 낮음).
Statement G13: We suggest regular abdominopelvic CT scan of 6~12 month interval for detection of extra-gastric recurrence after curative endoscopic resection of early gastric cancer based on absolute and expanded criteria (Grade of recommendation: weak, Level of evidence: low).
조기위암 내시경 절제술 후 복부 컴퓨터단층촬영술 추적검사에 대한 정립된 진료지침은 매우 부족하다. 일본의 진료지침에서는 확대 적응증에 해당하는 경우 전이 발견을 위하여 초음파 또는 컴퓨터단층촬영술을 6~12개월 간격으로 시행할 것을 권고하고 있으며[7,120], 유럽 진료지침에서는 확대 적응증 병변에 대하여 복부 컴퓨터단층촬영술을 고려할 수 있다고 하였다[1]. 2015년 발표된 국내의 한 연구에서는 절대 및 확대 적응증 환자 2명에서 완전 절제 후 각각 5년, 4년 뒤 림프절 전이가 발견되었다고 보고한 바가 있으며[101], 2017년에 발표된 국내 연구에서는 위강 외 재발이 발견된 15예 중 확대 적응증의 66.7% (4/6), 적응증 외의 83.3% (5/6)에서 위강 내 재발 없이 컴퓨터단층촬영술에서만 위강 외 재발이 발견되어, 확대 적응증 환자에서는 컴퓨터단층촬영술 추적검사가 필요하다고 제안하였다[194]. 그러나 다른 국내 연구에서는 절대 및 확대 적응증 환자의 내시경 완전 절제 후 시행한 2,182예의 복부 컴퓨터단층촬영술 검사에서 단지 2예(절대 적응증 1예 및 확대 적응증 1예)에서만 위강 외 림프절 재발이 발견되어 컴퓨터단층촬영술의 비용, 방사선량 등을 고려하면 확대 적응증 환자에서 내시경 완전 절제 후 컴퓨터단층촬영술 추적검사는 불필요하다고 제안하였다[195]. 또한, 내시경으로 완전 절제된 점막암 894예를 내시경 및 복부 컴퓨터단층촬영술로 추적검사한 결과, 역시 단 2예에서만 컴퓨터단층촬영술에서 의심 소견이 발견되어 내시경 치료 후 추적검사에서 컴퓨터단층촬영술의 역할은 미미하다고 보고하였다[196]. 따라서, 복부 컴퓨터단층촬영술 추적검사의 시행 대상, 간격 등은 아직 정확히 정립되어 있지 않으며 더 많은 논의와 연구가 필요하다.
조기대장암
1. 권고안 C1: 조기대장암에서 분화도가 나쁜 암(저분화선암, 반지세포암, 점액암), 깊은 점막하층 침범, 림프관 및 정맥 등의 맥관 침범 또는 침윤의 깊은 경계면에 중등도 이상의 종양 발아를 보이는 경우 국소 림프절 전이의 고위험 소견이다(권고등급: 강함, 근거수준: 중등도).
Statement C1: Poor histologic types (poorly differentiated adenocarcinoma, signet ring cell carcinoma, and mucinous carcinoma), deep submucosal invasion, lymphovascular invasion, and intermediate-to-high-grade tumor budding at the site of deepest invasion are risk factors of lymph node metastasis in early colorectal cancer (Grade of recommendation: strong, Level of evidence: moderate).
조기대장암의 잠재적인 림프절 전이 위험을 예측하는 것은 조기대장암을 내시경이나 외과적으로 국소 절제한 후 추가적으로 근치적 수술을 진행할 것인지 결정하는데 큰 영향을 미친다. 조직학적 분화도는 조기대장암에서 림프절 전이를 예측하는 가장 전통적 지표로, 분화도가 나쁜 암(저분화선암, 반지세포암, 점액암)은 분화도가 좋은 암(고분화/중등도분화 선암)에 비하여 림프절 전이의 위험이 높으며 분화도의 단계에 비례하여 전이가 증가한다[197-202]. 분화도에 따른 다변량 분석 결과들에서 조직학적으로 나쁜 분화(poorly differentiated adenocarcinoma, signet ring cell carcinoma, mucinous carcinoma)의 소견은 양호한 분화에 비하여 교차비가 약 2.93~45.9로 림프절 전이 위험이 증가하였다[203-205]. 4개의 메타분석 연구 결과에서도 분화도가 나쁜 조기대장암의 경우 교차비 4.78~8.27로 림프절 전이의 위험이 증가되었다[8,206-208].
분화도가 양호한 조기대장암 중 점막에 국한된 경우에는 림프절 전이를 일으키지 않으나 점막하층으로 침범이 있는 경우는 대략 6~20%에서 림프절 전이가 발생한다[8,206-209]. 점막하 침범의 상대적 깊이를 이용한 연구들에서 유경성 병변은 Haggitt 분류에 따르며, 비유경성 병변은 Kudo 또는 Kikuchi 분류에 따라 침범 깊이를 나누는데[210-212], 이들 분류 모두에서 점막하 침범의 상대적 깊이가 깊을수록(Haggitt level 4와 Kudo sm2~3) 림프절 전이의 위험도가 비례하여 높아진다[197-199,205,209,213,214]. 점막근판으로부터 점막하층의 침범 깊이를 직접 측정하여 림프절 전이 위험을 평가한 절대적 기준을 이용한 연구들에서는 비유경성 암종에서 수직 침범의 깊이가 1,000 μm 이상인 경우에 림프절 전이의 위험이 존재하며, 깊이가 깊을수록 위험도가 증가한다[201,203,215-219]. 점막하 침범 깊이 1,000 μm 이상을 기준으로 림프절 전이 위험을 분석한 메타연구들에서는 교차비가 약 3.0~5.93으로 전이 발생이 증가되었다[8,206-208]. 하지만 여러 연구들에서 이러한 점막하층으로의 절대적 침범 깊이 측정에 따른 전이 위험은 비교적 낮은 예측력을 보여 최근에는 이를 보완하기 위하여 침범의 가로 직경도 림프절 전이 예측의 정량적 측정인자로 함께 고려되고 있다[8,201].
맥관(림프관 및 정맥)으로의 암의 침범은 다변량 분석이 포함된 여러 연구들에서 국소 림프절로의 전이를 시사하는 독립적인 예측인자였다[198-205,220]. 과거의 연구들에서 림프관 침범 또는 정맥 침범에 따라서 림프절 전이 위험도가 다르게 보고되기도 하였으나 5개의 메타분석 연구에 따르면 림프절 전이에 있어 각각 단독으로 림프관 침범(OR=4.15~6.91)과 정맥 침범(OR=2.20~4.03)으로 분석한 경우와 둘을 하나의 범주인 맥관 침범(OR=3.9~5.47)으로 분석한 3가지 경우 모두 림프절 전이의 위험이 증가하는 것으로 나타났다[8,206-208,221].
종양 발아는 점막하 침윤의 깊은 경계면에 종양과 떨어진 단일의 암세포 또는 5개 미만의 암세포로 이루어진 군집이 있는 경우로 정의하며[222,223], 종양 발아의 기준은 연구마다 차이가 있으나 일반적으로 5개 이상의 종양 발아 소견이 관찰되는 경우를 중등도 이상의 종양 발아로 분류하며 림프절 전이의 위험이 증가하는 것으로 보고되고 있다[198,201,219,224,225]. 메타분석 연구들에 따르면 종양 발아의 존재는 교차비 3.26~7.74로 림프절 전이의 위험이 증가하는 것으로 나타났다[8,206-208,221,223]. 일본의 대규모 다기관 연구에서는 침윤 깊은 경계면에 저분화 세포군집(poorly differentiated clusters)을 보이는 경우도 림프절 전이를 예측하는 유용한 병리적 지표로 제시하고 있다[201,225]. 저분화 세포군집은 침윤면(invasive front)에서 관찰되는 선(gland) 구조를 형성하지 않는 5개 이상의 암세포로 이루어진 군집으로 정의하므로, 종양 발아에 비하여 그 크기가 커서 면역화학염색 없이 헤마톡실린-에오신(H&E) 염색으로 쉽게 관찰할 수 있다.
2. 권고안 C2: 림프절 전이 위험이 높은 점막하층암은 내시경 절제만 시행한 경우에는 수술에 비하여 재발률이 높으므로 내시경 절제 후 조직 소견에서 림프절 전이 고위험 소견이 확인되면 추가 수술을 권고한다(권고등급: 강함, 근거수준: 높음).
Statement C2: Endoscopic resection of submucosal colorectal cancer with a high risk of lymph node metastasis has a higher recurrence rate than surgical resection. Therefore, we recommend additional surgery if histological signs after endoscopic resection suggest a high risk of lymph node metastasis (Grade of recommendation: strong, Level of evidence: high).
대장의 점막층에 국한된 조기대장암은 림프절 전이가 없으므로 내시경 절제술로 원발 종양을 완전 절제하였다면 재발 가능성은 없고 치료는 종료된다. 미국의 인구 기반 연구에서는 점막 혹은 점막하 침윤 조기대장암의 경우(병기 1기 이하) 장경 4 cm 이하의 종양에서는 5년 생존율에 있어 내시경 치료와 수술적 치료 간의 차이가 없었다[226]. Mounzer 등[227]이 발표한 연구에서도 점막에 국한된 대장암의 치료에 있어 내시경 치료와 수술 치료의 5년 대장암 특이적 무재발 생존율(97.6% vs. 97.5%; P=0.75) 및 대장암 특이적 사망률(HR=1.10, 95% CI: 0.72~1.69; P=0.65)은 두 치료 사이에 차이가 없었다.
점막하 침윤 조기대장암에서는 내시경 치료를 한 경우 수술 치료보다 유의하게 낮은 무재발 생존율(89.8% vs. 96.6%; P<0.001)과 높은 대장암 특이적 사망률(HR=2.40, 95% CI: 1.75~3.29; P<0.001)을 보고하였다[227]. 점막하 침윤 조기대장암의 치료에 있어 내시경 절제와 수술 절제를 직접적으로 비교한 연구들에서 내시경 절제한 경우 국소 재발률은 2.3~6.4%[228-230], 수술 절제한 경우 국소 재발률은 0.9~1.87%로 수술을 시행한 경우에 재발률이 상대적으로 낮게 보고되었다[228-230]. 그런데, 이와 같은 예후의 차이는 림프절 전이 위험도가 낮은 점막하 침윤 조기대장암 인지 림프절 전이 위험도가 높은 점막하 침윤 조기대장암인지에 따라 달라진다. 2014년 국내의 한 연구에 의하면[231], 림프절 전이 저위험군인 점막 및 얕은 점막하 침윤 조기대장암의 경우 평균 37개월(6~98개월) 누적 재발률에 있어서 내시경 치료와 수술 치료 사이에 차이는 없었다(P=0.641). 5년 무재발 생존율에 있어서도 Yoda 등[232]은 저위험 점막하 침윤 대장암의 경우 98%로 매우 높은 결과를 보고하였다. 반면, 고위험인자를 동반한 조기대장암의 경우 림프절 전이율은 15.5%로 동반하지 않았던 경우에서의 7.1%에 비하여 유의하게 높은 결과를 보였다(P=0.001) [229] 일본의 다른 연구[232]에서도 고위험 점막하 침윤 조기대장암의 경우에는 통계학적으로 유의하지는 않았지만 내시경 치료 후 추가 수술을 시행한 군에서 추가 수술을 하지 않았던 군에 비하여 5년 무재발 생존율이 더 높았다(97% vs. 89%; P=0.130). 이후 발표된 연구들에서도 내시경 치료만으로 시술을 종료한 고위험인자 동반 조기대장암에서 높은 재발률을 보고하고 있으며[233], 생존율에 있어서도 추가적인 수술을 시행한 군에 비하여 유의하게 낮았다[234,235]. 따라서, 점막에 국한되어 있거나 림프절 전이의 고위험인자가 없는 조기대장암의 내시경 치료는 효과적이지만 고위험인자를 동반한 조기대장암의 경우 내시경 치료 후 추가적인 수술이 필요하다.
3. 권고안 C3: 조기대장암 내시경 절제 전에 깊은 점막하층 암의 가능성을 평가하기 위하여 선구 형태 및 혈관 형태 관찰을 권고한다(권고등급: 강함, 근거수준: 높음).
Statement C3: We recommend endoscopic assessment of pit patterns and vascular patterns to estimate the depth of submucosal invasion before endoscopic resection of early colorectal cancer (Grade of recommendation: strong, Level of evidence: high).
림프절 전이 고위험 소견을 보이는 점막하층암은 수술 치료가 필요하며, 림프절 전이 위험인자 중 점막하층 침범 깊이와 내시경 소견과의 연관성에 대하여 많은 연구가 수행되어 왔다. 조기대장암에서 치료 전 침범 깊이를 예측하는 것은 수술 또는 내시경 절제의 적절한 치료 방법을 결정하기 위하여 필수적이며, 색소확대내시경(magnifying chromoendoscopy)과 협대역영상(NBI)을 통하여 깊은 점막하층 침범을 예측할 수 있다.
Kudo에 의하여 제안된 선구 형태(pit pattern) 분석은 조기대장암의 점막하층 침범 예측에 유용하며, 색소확대내시경으로 관찰하였을 때 V형, 특히 VN형에 속하는 선구 형태를 보이면 깊은 점막하층까지 침범하였을 가능성이 높다(Table 5) [236-238]. 조기대장암 의심 병변의 선구 형태 분석을 통한 침범 깊이 예측 연구에 의하면 선구 형태가 IIIL, IIIS, IV형인 경우 각각 점막하층을 침범한 조기대장암의 빈도는 1%, 5%, 8%에 불과하였지만 VI형은 14%, VN형은 80%가 점막하층까지 침범한 암이었다[239]. 선구 형태가 깊은 점막하층 침범을 예측하는 민감도는 조기대장암의 육안 분류에 따라 다소 차이를 보이며, 융기형, 편평형, 함몰형에서 각각 깊은 점막하층 침범의 진단 정확도는 75.8%, 85.7%, 98.6%로 침범 깊이를 정확히 판단할 수 있어 조기대장암의 진단과 치료 방침 결정에 유용하다[240]. 깊은 점막하층암을 예측하는데 있어 색소확대내시경의 정확도에 대한 17개의 관찰 연구를 포함한 메타분석 결과에 의하면 민감도 81%, 특이도 95%였으며[15], 최근의 3개 초록을 포함한 9개 연구의 메타분석 결과에 있어서도 민감도 84%, 특이도 97%로[241], 이는 깊은 점막하층 침범을 판정하는데 색소확대내시경의 유용성을 시사하는 결과이다. 색소확대내시경 시 인디고카민과 크리스탈 바이올렛(crystal violet)이 주로 이용되며, 두 가지 염색법 사이에 진단 정확도 차이는 없었다[15].

협대역영상내시경은 표면 미세혈관 구조를 잘 파악할 수 있는 기법인데, 선구 형태가 깨져 있으면서 굵은 미세혈관이 불규칙하게 주행하거나 혈관 분포가 균일하지 않으면서 무혈관부(avascular area)가 관찰되는 경우에 깊은 점막하층까지 침범하였을 가능성이 높다[242-244]. 협대역영상내시경을 이용한 표면 미세혈관 형태 분류법으로 Sano 분류법과 Hiroshima 분류법 등이 초창기에 제시되었고, 이후 NBI International Colorectal Endoscopic (NICE) Classification, Japan NBI Expert Team Classification (JNET) 등의 분류법을 전문가 그룹에서 제시하였다(Table 6). 깊은 점막하층암과 점막암 또는 얕은 점막하층암을 감별하는데 있어 Sano 분류 IIIA/IIIB의 민감도, 특이도, 정확도는 각각 85%, 89%, 88%였다[245]. Hiroshima 분류 C3의 깊은 점막하층암 진단 민감도, 특이도, 정확도는 각각 67%, 99%, 93%이며, 관찰자 간 및 관찰자 내 일치도는 각각 kappa 값 0.749, 0.745로 우수하였다[246]. JNET 분류 type III의 깊은 점막하층암의 진단 민감도, 특이도, 정확도는 각각 55.4%, 99.8%, 96.6%였다[247,248]. 깊은 점막하층암을 예측하는데 있어 협대역영상내시경의 정확도에 대한 13개의 관찰 연구를 포함한 메타분석 결과에 의하면 민감도 77%, 특이도 98%였으며[15], 최근의 3개 초록을 포함한 17개 연구의 메타분석 결과에 있어서도 민감도 74%, 특이도 98%로[241] 조기대장암의 깊은 점막하층 침범 정도를 정확히 예측함을 시사하였다.

선구 형태나 표면 미세혈관 형태 외에도 병변의 단단함, 종양 표면의 깊고 불규칙한 함몰, 공기 주입에 따른 종양 형태의 변화가 없을 때, 병변 주위 점막주름이 집중되는 소견, 점막하층에 용액을 주입하였을 때 병변 아래 점막하층 부위가 잘 떠오르지 않는 non-lifting sign 등이 깊은 점막하층암을 시사하는 육안 소견으로 알려져 있다[249,250]. Non-lifting sign을 보이는 경우 점막하층의 섬유화나 깊은 점막하층 침범을 시사하는 것으로 알려져 있으나[251] 육안적 형태에 의한 깊은 점막하층암의 예측에 비하여 낮은 민감도 및 정확도를 보이는 것으로 보고되어[252] 아직까지 깊은 점막하층 침범 예측의 확실한 유용성에 대한 근거는 충분하지 않다. 깊은 점막하층암을 예측하는데 있어 육안적 형태의 정확도에 대한 6개의 관찰 연구를 메타분석한 결과 진단의 특이도는 80~98%였으나 민감도는 18~68%로, 이는 깊은 점막하층암을 예측하는 데에는 육안적 형태보다 색소확대내시경 및 협대역영상내시경이 우수함을 시사한다[15].
색소확대내시경과 협대역영상내시경의 깊은 점막하층암 예측 정확도를 비교 분석한 메타분석 연구에 의하면 두 가지 내시경 기법 사이에 민감도(색소확대내시경 81% vs. 협대역영상내시경 77%, P=0.41)와 특이도(95% vs. 98%, P=0.09)는 차이를 보이지 않았다. 반면, 최근 3개의 초록을 포함한 17개 연구의 메타분석에 의하면 색소확대내시경이 협대역영상내시경에 비하여 깊은 점막하층암 예측에 있어 특이도는 차이가 없었으나 민감도(84% vs. 74%, P<0.01)는 우월한 소견을 보였으며, 30명의 확대 및 영상강화내시경 전문가를 대상으로 한 설문 연구에서 깊은 점막하층암을 예측하는데 있어 색소확대내시경이 협대역영상내시경에 비하여 우월함(88% vs. 83%, P=0.013)을 보고하였다[253]. 하지만 현재까지의 연구는 한국 및 일본에서 이루어진 연구가 대부분이어서 추가 연구가 필요하다.
결론적으로, 내시경의 육안 소견에서 깊은 점막하층암을 시사하는 소견이 있거나 Kudo 선구 형태가 VN형인 경우, 협대역영상내시경상 Sano 분류 IIIB, Hiroshima 분류 C3, JNET 분류 3에 해당하는 경우에는 깊은 점막하층 침범의 가능성이 높으므로 외과 수술을 우선적으로 고려해야 한다. 한편, 선구 형태나 협대역영상내시경 소견은 깊은 점막하층 침범을 진단함에 있어 특이도는 매우 우수하나 민감도는 상대적으로 낮으며, 진단 정확도도 비교적 우수하지만 조직병리 소견을 대체할 만한 수준은 아니므로, 깊은 점막하층 침범을 시사하는 내시경 소견을 보이는 병변이라 하더라도 내시경으로 안전하고 쉽게 절제할 수 있는 형태의 병변은 내시경 절제 후 조직병리 소견을 바탕으로 추가 수술의 필요성을 결정할 수도 있다.
4. 권고안 C4: 조기대장암 추정 또는 확진 병변을 내시경으로 치료할 때에는 일괄 절제를 통한 조직학적 완전 절제를 목표로 해야 한다. 내시경 절제의 적응은 되나 내시경 점막 절제술로는 일괄 절제가 어려운 조기대장암에 대해서는 내시경 점막하 박리술을 시행할 것을 권고한다(권고등급: 강함, 근거수준: 중등도).
Statement C4. En bloc and histologically complete resection should be achieved for endoscopic treatment of a suspected or established early colorectal cancer. We recommend endoscopic submucosal dissection for the treatment of endoscopically resectable early colorectal cancer which cannot be resected en bloc using endoscopic mucosal resection technique (Grade of recommendation: strong, Level of evidence: moderate).
조기대장암에서 깊은 점막하층 침범, 분화도가 나쁜 조직형(poorly differentiated adenocarcinoma, signet ring cell carcinoma, mucinous carcinoma), 암세포의 맥관 침범, 종양 발아 또는 저분화 세포군집 등은 조기대장암의 림프절 전이와 관련된 위험인자이며, 내시경 절제 후 병리 소견에서 이러한 소견이 관찰되면 추가적인 수술이 필요하다. 또한, 수직 절제연에 암세포 양성으로 관찰되는 등의 조직학적으로 불완전 절제된 점막하층암도 추가적인 수술이 필요하다. 따라서, 조기대장암의 내시경 치료에 있어서 일괄 절제는 조직학적 완전 절제율을 높임과 동시에 정확한 병리 소견을 확인함으로써 추가 수술 필요성을 판단하는데 매우 중요하다[49,254-260]. Fujiya 등[257]은 2015년도에 대장 병변의 내시경 절제 방법인 점막하 박리술과 점막절제술을 비교한 연구들을 메타분석하여 일괄 절제율이 점막하 박리술은 91.7%, 점막절제술은 46.7%, 교차비 6.84 (95% CI: 3.30~14.18)로 점막하 박리술의 일괄 절제율이 점막절제술에 비하여 높다고 보고하였다. 또한 같은 연구에서 완전 절제율도 점막하 박리술 시 80.3%, 점막절제술 시 42.3%, 교차비 4.26 (95% CI: 3.77~6.57)으로 점막하 박리술의 완전 절제율이 점막절제술에 비하여 유의하게 높았다. 2016년 Arezzo 등[258]도 20 mm 이상의 무경성 대장 병변에 대하여 점막하 박리술과 점막절제술을 비교한 연구들을 메타분석하여 일괄 절제율이 점막하 박리술 89.9%, 점막절제술 34.9%로 상대 위험도 1.93 (95% CI: 1.46~2.54)으로 확인하였고, 근치적 절제율 역시 점막하 박리술 79.6%, 점막절제술 36.2%로 상대 위험도 2.01 (95% CI: 1.76~2.29)로 확인하여 20 mm 이상의 무경성 대장병변의 내시경 절제 시 점막하 박리술이 일괄 절제 및 근치적 절제에 점막절제술보다 우월함을 보고하였다.
대장 폴립절제술 시 발생 가능한 출혈이나 천공 등의 합병증은 보고마다 다양한데, 한 메타분석에서 천공 발생률은 점막하 박리술이 4.0~5.7%로 점막절제술의 0.8~1.4%보다 더 높았다[257-259]. 한편, 점막하 박리술 후 발생한 합병증의 대부분이 내시경으로 치료 가능하고, 점막하 박리술 후 합병증 발생으로 인한 수술 빈도는 전체 병변 중 1% 정도에 불과하여 점막하 박리술의 안전성은 수용할 수 있는 수준으로 여겨진다[261]. 그러나 대장 병변에 대한 점막하 박리술은 시술의 난이도가 높아 시술자의 숙련도에 따라 합병증 발생률 및 일괄 혹은 완전 절제율 등의 결과가 현저하게 차이가 난다[262,263]. 따라서, 대장의 내시경 점막하 박리술은 적절한 수련 후 충분한 경험을 가진 치료 내시경 전문가가 시술 관련 합병증에 의한 응급상황에 대처 가능한 의료기관에서 시행해야 한다[262-266].
결론
조기위장관암에서 내시경 절제술은 수술적 절제에 비하여 이상 반응이 적고 재원 기간이 짧으며, 비용이 낮으면서 장기를 보존할 수 있다는 장점이 있다. 그러나 모든 조기위장관암 환자가 내시경 절제술의 적응증이 되는 것은 아니므로, 내시경 절제술로 치료 가능한 적절한 조기위장관암 환자를 선별하여 시술하는 것이 중요하다. 또한, 내시경 절제술 후 수술 치료나 정기적인 추적 관찰 등 적절한 관리가 이어져야 내시경 절제술의 우수한 장기 치료 성적을 보장할 수 있다. 이 임상진료지침은 내시경 절제술을 시행하는 소화기내시경 의사에게 표준적인 진료 과정을 제시함으로써 과잉 진료나 부적절한 진료를 다소나마 예방할 수 있을 것으로 생각하며, 장기적으로 조기위장관암의 치료에 있어서 내시경 절제술의 보급 및 확산에도 기여할 수 있으리라 기대한다.
Notes
No potential conflict of interest relevant to this article was reported.
Supplementary Materials
PICOs for Each Statement
Search Flow Charts