ņä£ ļĪĀ
1980ļģäļīĆ ņ┤ł, MarshallĻ│╝ Warren [1]ņØ┤ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼Ļ░Ć ņ£äņŚ╝ņØś ņøÉņØĖņ×äņØä ļ░ØĒ×ī ņØ┤Ēøä, Ēśäņ×¼Ļ╣īņ¦Ć ņ£äĻČżņ¢æ, ņŗŁņØ┤ņ¦ĆņןĻČżņ¢æ, ņ£ä ņĀÉļ¦ēĻ┤ĆļĀ©ļ”╝ĒöäņĪ░ņ¦ü(mucosa-associated lymphoid tissue) ļ”╝Ēöäņóģ ļō▒ ļŗżņ¢æĒĢ£ ņ£ä, ņŗŁņØ┤ņ¦Ćņן ņ¦łĒÖśĻ│╝ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ņØś ņŚ░Ļ┤Ćņä▒ņØ┤ ņĢīļĀżņĪīļŗż[2]. ĒŖ╣Ē׳ ņŚ¼ļ¤¼ ņŚŁĒĢÖ ņŚ░ĻĄ¼ņŚÉņä£, ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ņÖĆ ņ£äņĢöĻ│╝ņØś ļÜ£ļĀĘĒĢ£ ņŚ░Ļ┤Ćņä▒ņØ┤ ļ░ØĒśĆņ¦Ćļ®┤ņä£ 1994ļģäņŚÉ ņäĖĻ│äļ│┤Ļ▒┤ĻĖ░ĻĄ¼ ņé░ĒĢś International Agency for Research on CancerņŚÉņä£ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ļź╝ ņĀ£1ĻĄ░ ļ░£ņĢöļ¼╝ņ¦łļĪ£ ĻĘ£ņĀĢĒĢśņśĆļŗż[3]. ĻĘĖļ¤¼ļéś ņ£äņĢö ļ░£ņāØņŚÉļŖö ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņÖĖņŚÉ ņŚ░ļĀ╣, ņä▒ļ│ä, ĒØĪņŚ░, ņ£äņĢö Ļ░ĆņĪ▒ļĀź, ĒøłņĀ£ Ēś╣ņØĆ ņĀłņØĖ ņØīņŗØ, ļé«ņØĆ ņé¼ĒÜīĻ▓ĮņĀ£ņĀü ņłśņżĆ ļō▒ ņŚ¼ļ¤¼ ņØĖņ×ÉĻ░Ć Ļ┤ĆņŚ¼ĒĢśļ®░[4], ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņ×Éņ▓┤ļŖö ņ£äņĢöņØä ņØ╝ņ£╝ĒéżļŖö ņ¦üņĀæņĀüņØĖ ņøÉņØĖņØ┤ ņĢäļŗÉņ¦ĆļÅä ļ¬©ļźĖļŗżļŖö ņØśĻ▓¼ļÅä ņĀ£ņŗ£ļÉśĻ│Ā ņ׳ļŗż[5,6].
ņØ┤ņŚÉ ļö░ļØ╝ ļ¦ÄņØĆ ņŚ░ĻĄ¼ņ×ÉļōżņØ┤ ņ£äņĢöņØś ļśÉ ļŗżļźĖ ņøÉņØĖņØä ĻĘ£ļ¬ģĒĢśļĀżĻ│Ā ņŗ£ļÅäĒĢśĻ│Ā ņ׳ņ£╝ļ®░, ņØ┤ ņżæ Ļ░Ćņן ļīĆĒæ£ņĀüņØĖ Ļ▓āņØ┤ ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æ(microbiota)ņØ┤ļŗż[7]. ļ»ĖņāØļ¼╝ņŚÉ ļīĆĒĢ£ ņŚ░ĻĄ¼ļŖö ņĀäĒåĄņĀüņ£╝ļĪ£ 100ļģä ļäśĻ▓ī ļ░░ņ¢æļ▓ĢņØä ĒåĄĒĢ┤ ņØ┤ļŻ©ņ¢┤ņĪīņ£╝ļéś, 2000ļģäļīĆ ņ┤łļ░ś ņ░©ņäĖļīĆ ņŚ╝ĻĖ░ņä£ņŚ┤ļČäņäØļ▓Ģ(next-generation sequencing)ņØ┤ ļÅäņ×ģļÉśļ®┤ņä£ Ēśäņ×¼ļŖö ļ»ĖņāØļ¼╝ņØś DNA ņä£ņŚ┤ ļČäņäØņØä ĻĖ░ļ░śņ£╝ļĪ£ ĒĢ£ ļ╣äļ░░ņ¢æļ▓ĢņØ┤ ļ»ĖņāØļ¼╝ ņŚ░ĻĄ¼ ļ░®ļ▓Ģņ£╝ļĪ£ ļäÉļ”¼ ĒÖ£ņÜ®ļÉśĻ│Ā ņ׳ļŗż[7,8]. Ēśäņ×¼ļŖö, ņ£ä ļé┤ņŚÉļÅä ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņÖĖņŚÉ ņŚ¼ļ¤¼ ļ»ĖņāØļ¼╝ņØ┤ ņāüņ×¼ĒĢśĻ│Ā ņ׳ņØīņØä ņĢīĻ│Ā ņ׳ņ£╝ļ®░, ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņÖĖņŚÉ ņ£äņĢöĻ│╝ ņŚ░Ļ┤ĆļÉ£ ļ░ĢĒģīļ”¼ņĢäļź╝ ĻĘ£ļ¬ģĒĢśĻ│Āņ×É ĒĢśļŖö ļģĖļĀźņØ┤ ņ׳ņŚłļŗż[8,9]. ĒŖ╣Ē׳, ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ļ│ĆĒÖöĒĢśļŖö ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ĒŖ╣ņä▒ņØä ĒīīņĢģĒĢśļĀżļŖö ņŚ░ĻĄ¼Ļ░Ć ļŗżņłś ņ¦äĒ¢ēļÉśņŚłļŗż[6,10-16]. ņØ┤ņŚÉ ļ│ĖĻ│ĀņŚÉņä£ļŖö ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī ņĀä/Ēøä ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØä ĒŖ╣ņä▒ņØä ļ╣äĻĄÉĒĢ┤ļ│┤Ļ│Ā ņ£äņČĢņä▒ņ£äņŚ╝ ļ░Å ņןņāüĒö╝ĒÖöņāØ, Ēś╣ņØĆ ņ£äņĢöņØś ļ░£ļ│æĻ│╝ ņŚ░Ļ┤ĆļÉśļŖö ļ░ĢĒģīļ”¼ņĢäņŚÉ ļīĆĒĢ┤ ņé┤ĒÄ┤ļ│┤Ļ│Āņ×É ĒĢ£ļŗż.
ļ│Ė ļĪĀ
1. ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ░ÉņŚ╝ņ£╝ļĪ£ ņØĖĒĢ£ ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļŗżņ¢æņä▒ ļ│ĆĒÖö
ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØ┤ ņ¦łļ│æņŚÉ ļ»Ėņ╣śļŖö ņśüĒ¢źņØä ņØ┤ĒĢ┤ĒĢĀ ļĢī Ļ░Ćņן ņżæņÜöĒĢ£ Ļ▓ā ņżæ ĒĢśļéśļŖö ĒŖ╣ņĀĢ ĒÖśĻ▓ĮņŚÉ ņĪ┤ņ×¼ĒĢśļŖö ļ»ĖņāØļ¼╝ņØś ļŗżņ¢æņä▒ņØ┤ļŗż[17]. ņןļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļŗżņ¢æņä▒ņØĆ Ļ▒┤Ļ░ĢņØĖļ│┤ļŗż ņŚ╝ņ”Øņä▒ ņןņ¦łĒÖś ĒÖśņ×Éļéś Clostridioides difficle ņŚ░Ļ┤Ć ņןņŚ╝ ĒÖśņ×ÉņŚÉņä£ ļŹö ļé«ņ£╝ļ®░, ņØ╝ļ░śņĀüņ£╝ļĪ£ ņ¦łļ│æņØ┤ ļ░£ņāØĒĢĀ Ļ▓ĮņÜ░ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļŗżņ¢æņä▒ņØ┤ ļé«ņĢäņ¦ĆļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[17,18]. ĻĘĖļ¤¼ļéś ņäĖĻĘĀņä▒ ņ¦łņŚ╝ ĒÖśņ×ÉņØś ņ¦ł ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØĆ Ļ▒┤Ļ░ĢņØĖņØś ņ¦ł ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņŚÉ ļ╣äĒĢ┤ ņśżĒ׳ļĀż ļŗżņ¢æņä▒ņØ┤ ļåÆĻĖ░ ļĢīļ¼ĖņŚÉ ļŗżņ¢æņä▒ņØś ņ”ØĻ░ĆĻ░Ć ļ░śļō£ņŗ£ Ļ▒┤Ļ░ĢĒĢ£ ņāüĒā£ļź╝ ņØśļ»ĖĒĢśļŖö Ļ▓āņØĆ ņĢäļŗłļŗż[19].
ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ņŚÉ Ļ░ÉņŚ╝ļÉśņ¦Ć ņĢŖņØĆ Ļ▒┤Ļ░ĢņØĖņØś ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņŚÉļŖö Firmicutes, Proteobacteria, Cyanobacteria, Bacteroidetes, Actinobacteria, Acidobacteria ļō▒ ļŗżņ¢æĒĢ£ phylumņØ┤ Ļ┤Ćņ░░ļÉśļ®░, ļŗżņ¢æņä▒ ņŚŁņŗ£ ļåÆņØĆ ņłśņżĆņØ┤ļŗż[11,13]. ļ░śļ®┤, ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ņŚÉ Ļ░ÉņŚ╝ļÉ£ ĒÖśņ×ÉņØś Ļ▓ĮņÜ░ ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æ ņżæ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ņØś ņāüļīĆ ĒÆŹļČĆļÅä(relative abundance)ļŖö 90% ņØ┤ņāüņØ┤ļ®░[13], ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ņØś ņāØĒā£ņĀü ņ¦Ćņ£äĻ░Ć ņś¼ļØ╝Ļ░ÉņŚÉ ļö░ļØ╝ ņ×Āņ×¼ņĀüņ£╝ļĪ£ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ņÖĆ Ļ▓Įņ¤üĒĢĀ ņłś ņ׳ļŖö ļŗżļźĖ ļ»ĖņāØļ¼╝ņØś ņä£ņŗØ Ļ░ĆļŖźņä▒ņØ┤ ņżäņ¢┤ļōżĻ│Ā, Ļ▓░Ļ│╝ņĀüņ£╝ļĪ£ ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļŗżņ¢æņä▒ņØĆ ļ¦żņÜ░ ļé«ņĢäņ¦äļŗż[11,15]. ĻĘĖļ¤¼ļéś ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ░ÉņŚ╝ņØ┤ ņ¦ĆņåŹļÉ©ņŚÉ ļö░ļØ╝ ņ£äņČĢņä▒ ņ£äņŚ╝ ļ░Å ņןņāüĒö╝ĒÖöņāØņØ┤ ņ¦äĒ¢ēļÉśļ®┤ ņ£äņé░ ļČäļ╣äĻ░Ć ņżäņ¢┤ļōżļ®░ ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ņĪ░ņä▒ņØ┤ ļ│ĆĒÖöĒĢ£ļŗż. ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ņØś ņāüļīĆ ĒÆŹļČĆļÅäļŖö ņżäņ¢┤ļōżĻ│Ā, non-Helicobacter Proteobacteriaļź╝ ļ╣äļĪ»ĒĢśņŚ¼ ņŚ¼ļ¤¼ ļ░ĢĒģīļ”¼ņĢä ļČäļźśĻĄ░(taxa)ņØ┤ ļŖśņ¢┤ļéśļ®░, ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļŗżņ¢æņä▒ņØ┤ ļåÆņĢäņ¦äļŗż[11,13,15]. ņ”ē, ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØĆ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ļ»ĖĻ░ÉņŚ╝ ņāüĒā£ņŚÉņä£, ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ░ÉņŚ╝, ņ£äņČĢņä▒ ņ£äņŚ╝, ņןņāüĒö╝ĒÖöņāØņØ┤ ņ¦äĒ¢ēļÉ©ņŚÉ ļö░ļØ╝ ļŗżņ¢æņä▒ņØ┤ ņżäņ¢┤ļōżņŚłļŗżĻ░Ć ļŗżņŗ£ ļŖśņ¢┤ļéśļŖö ļÅÖņĀü ļ│ĆĒÖöļź╝ Ļ▓¬Ļ▓ī ļÉ£ļŗż.
2. ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻīņŚÉ ļö░ļźĖ ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļŗżņ¢æņä▒ ļ│ĄņøÉĻ│╝ ņĪ░ņä▒ ļ│ĆĒÖö
ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī ņŗ£ ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļŗżņ¢æņä▒ņØ┤ ļ│ĄņøÉļÉ£ļŗżļŖö Ļ▓āņØĆ ņŚ¼ļ¤¼ ņŚ░ĻĄ¼ņŚÉņä£ ļ░ØĒśĆņĀĖ ņ׳ļŗż(Table 1). ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ņ£ä ļé┤ ļ»ĖņāØļ¼╝ņØś ļ│ĆĒÖöļź╝ ļ╣äļ░░ņ¢æļ▓Ģņ£╝ļĪ£ ņ▓śņØī ĒÖĢņØĖĒĢ£ Ļ▓āņØĆ 2016ļģä ļ░£Ēæ£ļÉ£ Li ļō▒[10]ņØś ņŚ░ĻĄ¼ļĪ£, ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ░ÉņŚ╝ņØ┤ ļÅÖļ░śļÉ£ ņŗŁņØ┤ņ¦ĆņןĻČżņ¢æ ĒÖśņ×É 21ļ¬ģņŚÉ ļīĆĒĢ┤ ņĀ£ĻĘĀ ņ╣śļŻī ņĀä/Ēøä, 16S rRNA ņ£ĀņĀäņ×ÉņŚÉ ļīĆĒĢ┤ ņĀĢļ¤ē ņŗżņŗ£Ļ░ä ņżæĒĢ®ĒÜ©ņåī ņŚ░ņćäļ░śņØæļ▓Ģ(quantitative real-time polymerase chain reaction)ņØä ņŗ£Ē¢ēĒĢśņŚ¼ ņ£ä ļé┤ ņŻ╝ņÜö ļ»ĖņāØļ¼╝ņØś ņ¢æņØä ņĖĪņĀĢĒĢśņśĆļŗż. ņĀ£ĻĘĀ ņ╣śļŻī Ēøä, ņ£ä ņĀäņĀĢļČĆņŚÉņä£ Lactobacillus, Clostridium leptum, EnterobacteriaņØś ĒÆŹļČĆļÅäĻ░Ć ņ”ØĻ░ĆĒĢśņśĆĻ│Ā, Clostridium coccoidesņØś ĒÆŹļČĆļÅäļŖö Ļ░ÉņåīĒĢśņśĆļŗż. ņ£ä ņ▓┤ļČĆņŚÉņä£ļÅä LactobacillusņØś ĒÆŹļČĆļÅäļŖö ņ”ØĻ░ĆĒĢ£ ļ░śļ®┤ Clostridium coccoidesņØś ĒÆŹļČĆļÅäļŖö Ļ░ÉņåīĒĢśņśĆļŗż. ļŗżļ¦ī, ņØ┤ ņŚ░ĻĄ¼ļŖö ņżæĒĢ®ĒÜ©ņåī ņŚ░ņćäļ░śņØæļ▓ĢņØä ņØ┤ņÜ®ĒĢśņŚ¼ ļ¬®Ēæ£ļĪ£ ņé╝ņØĆ ņØ╝Ļ│▒ Ļ░Ćņ¦Ć ļ░ĢĒģīļ”¼ņĢä ĻĄ░ņŚÉ ļīĆĒĢ┤ņä£ļ¦ī ņŚ░ĻĄ¼ļź╝ ņ¦äĒ¢ēĒĢśņśĆĻĖ░ ļĢīļ¼ĖņŚÉ, ņŚ░ĻĄ¼ ļīĆņāüņØ┤ ņĢäļŗī ļŗżļźĖ ļ░ĢĒģīļ”¼ņĢäņØś ĒÆŹļČĆļÅäļéś ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļŗżņ¢æņä▒ņØä ĒÖĢņØĖĒĢĀ ņłśļŖö ņŚåņŚłļŗż. ļśÉĒĢ£, ņŗŁņØ┤ņ¦ĆņןĻČżņ¢æ ĒÖśņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ ĒĢśņśĆĻĖ░ ļĢīļ¼ĖņŚÉ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī ņØ┤Ēøä ņ¢æņä▒ņ×ÉĒÄīĒöäņ¢ĄņĀ£ņĀ£ļź╝ 2ņŻ╝Ļ░ä ņČöĻ░ĆļĪ£ Ēł¼ņĢĮĒĢśņśĆĻ│Ā, ļö░ļØ╝ņä£ ņ¢æņä▒ņ×ÉĒÄīĒöäņ¢ĄņĀ£ņĀ£ļĪ£ ņØĖĒĢ£ ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æ ņĪ░ņä▒ ļ│ĆĒÖö Ļ░ĆļŖźņä▒ņØä ņÖäņĀäĒ׳ ļ░░ņĀ£ĒĢĀ ņłś ņŚåņŚłļŗżļŖö ĒĢ£Ļ│äĻ░Ć ņ׳ļŗż.
2017ļģä Li ļō▒[11]ņØĆ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī ņĀä/Ēøä ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ņĪ░ņä▒ ļ│ĆĒÖöļź╝ ņĄ£ņ┤łļĪ£ 16S rRNA ņ£ĀņĀäņ×É ņŗ£ĒĆĆņŗ▒ņØä ĒåĄĒĢ┤ ļČäņäØĒĢśņśĆļŗż. ņ£äņŚ╝ ĒÖśņ×É 7ļ¬ģ, ņןņāüĒö╝ĒÖöņāØ ĒÖśņ×É 4ļ¬ģņŚÉ ļīĆĒĢ┤ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢ£ Ļ▓░Ļ│╝ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļŗżņ¢æņä▒ņØ┤ ņ”ØĻ░ĆĒĢśņśĆļŗż. ĒÆŹļČĆļÅäĻ░Ć ļŖśņ¢┤ļé£ ļ░ĢĒģīļ”¼ņĢä ļČäļźśĻĄ░ņØĆ ļīĆļČĆļČä non-Helicobacter ProteobacteriaņśĆļŖöļŹ░, Neisseria, Serratia, Haemophilus parainfluenzae, Rhizobium ļō▒ņØ┤ ņ׳ņŚłĻ│Ā, ņØ┤ ņÖĖņŚÉ Flavobacterium, Fusobacterium ļō▒ļÅä ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ĒÆŹļČĆļÅäĻ░Ć ņ”ØĻ░ĆĒĢśņśĆļŗż. ņØ┤ ņŚ░ĻĄ¼ļŖö ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ░ÉņŚ╝ņ£╝ļĪ£ ņØĖĒĢ┤ Ļ░ÉņåīļÉ£ ļŗżņ¢æņä▒ņØ┤ ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ļ│ĄņøÉļÉĀ ņłś ņ׳ņØīņØä ļ│┤ņŚ¼ņżĆ ņ▓½ ļ▓łņ¦Ė ņŚ░ĻĄ¼ņØ┤ĻĖ░ļŖö ĒĢśļéś, ņĀ£ĻĘĀ ņ╣śļŻī ļīĆņāüĻĄ░ņŚÉ ļŗ©ņł£ ņ£äņŚ╝ ĒÖśņ×ÉņÖĆ ņןņāüĒö╝ĒÖöņāØ ĒÖśņ×ÉĻ░Ć ņä×ņŚ¼ ņ׳ņ¢┤ ņĀ£ĻĘĀ ņ╣śļŻīņØś ĒÜ©Ļ│╝ļź╝ ņś©ņĀäĒ׳ ņØ┤ĒĢ┤ĒĢśĻĖ░ņŚÉļŖö ņĀ£ņĢĮņØ┤ ņ׳ņØä ņłś ņ׳ļŗż.
2019ļģä He ļō▒[12]Ļ│╝ Park ļō▒[13]ņØĆ ņ£äņČĢņä▒ ņ£äņŚ╝ ļ░Å ņןņāüĒö╝ĒÖöņāØņØ┤ ļ░£ņāØĒĢśņ¦Ć ņĢŖņØĆ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņŚ░Ļ┤Ć ņ£äņŚ╝ ĒÖśņ×ÉņŚÉ ļīĆĒĢ┤ņä£ ņĀ£ĻĘĀ ņ╣śļŻī ņĀä/Ēøä ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļ│ĆĒÖöļź╝ ļČäņäØĒĢśņśĆļŗż. He ļō▒[12]ņØś ņŚ░ĻĄ¼ņŚÉņä£ļŖö ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī ņĀäņŚÉ ļ╣äĒĢ┤ ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļŗżņ¢æņä▒ņØ┤ ņ”ØĻ░ĆĒĢ©ņØä ļ│┤ņśĆĻ│Ā, ņĀ£ĻĘĀ ņ╣śļŻī Ēøä 26ņŻ╝ Ļ▓ĮĻ│╝ ņŗ£ ņĀ£ĻĘĀ ņ╣śļŻī ņĀäņŚÉ ļ╣äĒĢ┤ Prevotella, Ralstonia, Pseudomonas, LactobacillusņØś ĒÆŹļČĆļÅäĻ░Ć ņ”ØĻ░ĆĒĢ©ņØä ļ│┤ņśĆļŗż. ņĀ£ĻĘĀ ņ╣śļŻī Ēøä 4ņŻ╝ņÖĆ 24ņŻ╝ Ļ▓ĮĻ│╝ĒĢ£ ļÆż Ļ░üĻ░ü ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØä ļČäņäØĒĢśņśĆļŖöļŹ░, RalstoniaļŖö 24ņŻ╝ņ¦ĖņŚÉ ļ╣äĒĢ┤ 4ņŻ╝ņ¦ĖņŚÉ ĒÆŹļČĆļÅäĻ░Ć ļåÆņĢśĻ│Ā, PseudomonasļŖö 4ņŻ╝ņ¦ĖņÖĆ 24ņŻ╝ņ¦ĖņŚÉ ĒÆŹļČĆļÅä ņ░©ņØ┤Ļ░Ć ņŚåņŚłĻ│Ā, Prevotella, LactobacillusļŖö 4ņŻ╝ņ¦ĖņŚÉ ļ╣äĒĢ┤ 24ņŻ╝ņ¦ĖņŚÉ ĒÆŹļČĆļÅäĻ░Ć ļŹö ļåÆņĢä, ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ļŖśņ¢┤ļéśļŖö ļ░ĢĒģīļ”¼ņĢä ļČäļźśĻĄ░ļÅä ņŗ£ĻĖ░ņŚÉ ļö░ļØ╝ ļŗ¼ļØ╝ņ¦ł ņłś ņ׳ņØīņØä ļ│┤Ļ│ĀĒĢśņśĆļŗż. Park ļō▒[13]ņØĆ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī Ēøä Rhizobiales, Neisseriaceae ļō▒ņØś ĒÆŹļČĆļÅäĻ░Ć ņ”ØĻ░ĆĒĢ©ņØä ļ│┤ņśĆļŗż. ļŗżļźĖ ņŚ░ĻĄ¼ņÖĆ ļ¦łņ░¼Ļ░Ćņ¦ĆļĪ£ ņĀ£ĻĘĀ ņ╣śļŻī ņĀäņŚÉ ļ╣äĒĢ┤ ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ņĪ░ņä▒ņØ┤ Ēü¼Ļ▓ī ļ│ĆĒÖöĒĢśņśĆņ£╝ļéś, ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ņĪ░ņä▒ņØ┤ Firmicutes ļ░Å CyanobacteriaņØś ĒÆŹļČĆļÅäĻ░Ć ņāüļīĆņĀüņ£╝ļĪ£ ļåÆņØĆ Ļ▒┤Ļ░ĢņØĖņØś ļ»ĖņāØļ¼╝ĻĄ░ņ¦æļ│┤ļŗżļŖö Proteobacteria ļ░Å BacteroidetesņØś ĒÆŹļČĆļÅäĻ░Ć ņāüļīĆņĀüņ£╝ļĪ£ ļåÆņØĆ ņןņāüĒö╝ĒÖöņāØ ĒÖśņ×ÉņØś ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņŚÉ Ļ░ĆĻ╣ØĻ▓ī ļ│ĆĒÖöĒĢ©ņØä ĒÖĢņØĖĒĢśņśĆļŗż[13]. ņØ┤ļŖö ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ░ÉņŚ╝ņØä ņ╣śļŻīĒĢśļŹöļØ╝ļÅä ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ņĪ░ņä▒ņØ┤ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ░ÉņŚ╝ ņĀä ņāüĒā£ļĪ£ ņÖäņĀäĒ׳ ļ│ĄņøÉļÉśņ¦ĆļŖö ņĢŖņØä ņłśļÅä ņ׳ņØīņØä ņŗ£ņé¼ĒĢśļ®░, ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻīļ¦īņ£╝ļĪ£ ņ£äņĢöņØä 100% ņśłļ░®ĒĢĀ ņłś ņŚåļŖö ņØ┤ņ£ĀĻ░Ć ļÉĀ ņłśļÅä ņ׳ļŗż.
2019ļģä Serrano ļō▒[14]ņØś ņŚ░ĻĄ¼ņÖĆ 2020ļģä Miao ļō▒[16]ņØś ņŚ░ĻĄ¼ļŖö ņåīņĢä ĒÖśņ×ÉņŚÉņä£ņØś ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æ ņĪ░ņä▒ ļ│ĆĒÖöļź╝ ļČäņäØĒĢśņśĆļŗż. ņåīņĢäņŚÉņä£ņØś ņŚ░ĻĄ¼ļŖö ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ļ¦īņä▒ Ļ░ÉņŚ╝ņØś ņ£Āļ│æ ĻĖ░Ļ░äņØ┤ ĻĖĖņ¦Ć ņĢŖņØä Ļ▓ĮņÜ░ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻīņŚÉ ļö░ļźĖ ņ£äņĢö ļ░£ņāØ ņśłļ░® ĒÜ©Ļ│╝Ļ░Ć Ēü┤ ņłś ņ׳ļŗżļŖö Ļ░ĆņĀĢĒĢśņŚÉ, ņ£äņĢö ņśłļ░®ņŚÉ ļÅäņøĆņØ┤ ļÉśļŖö ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ĒŖ╣ņä▒ņØä ĒīīņĢģĒĢśļŖöļŹ░ ļÅäņøĆņØä ņżä ņłś ņ׳ļŗż. Serrano ļō▒[14]ņØĆ ņśżņŗ¼Ļ│╝ ļ│ĄļČĆļČłĒÄĖĻ░ÉņØä ĒśĖņåīĒĢśļŖö 7ļ¬ģņØś 13ņäĖ ņØ┤ĒĢś ņåīņĢä ĒÖśņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ ņĀ£ĻĘĀ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢśņŚ¼, ņĀ£ĻĘĀ ņ╣śļŻī ņĀäņŚÉ ļ╣äĒĢ┤ ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļŗżņ¢æņä▒ņØ┤ ņ”ØĻ░ĆĒĢśĻ│Ā, ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ░ÉņŚ╝ņØ┤ ņŚåļŖö ņåīņĢäņÖĆ ņĀ£ĻĘĀ ņ╣śļŻīļź╝ ļ░øņØĆ ņåīņĢä Ļ░äņŚÉ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļŗżņ¢æņä▒ņŚÉ ņ░©ņØ┤Ļ░Ć ņŚåņØīņØä ļ│┤ņśĆļŗż. ņĀ£ĻĘĀ ņ╣śļŻī ĒøäņØś ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņŚÉļŖö Pseudomonadaceae, Delftia, Kocuria, Stenotrophomonas ļō▒ņØś ĒÆŹļČĆļÅäĻ░Ć ņ”ØĻ░ĆĒĢśņśĆļŗż. Miao ļō▒[16]ņØś ņŚ░ĻĄ¼ņŚÉņä£ļŖö ĒÅēĻĘĀ 11ņäĖņØś ņåīņĢä ĒÖśņ×É 11ļ¬ģņŚÉ ļīĆĒĢ┤ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢśņśĆĻ│Ā, ņĀ£ĻĘĀ ņ╣śļŻī ņĀäņŚÉ ļ╣äĒĢ┤ ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļŗżņ¢æņä▒ņØ┤ ņ”ØĻ░ĆĒĢśņśĆņ£╝ļ®░ Neisseria, Curvibacter, HaemophilusņØś ĒÆŹļČĆļÅäĻ░Ć ņ”ØĻ░ĆĒĢśņśĆļŗż. ļśÉĒĢ£, ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ░ÉņŚ╝ņØ┤ ņŚåļŖö ņåīņĢäņÖĆ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻīļź╝ ļ░øņØĆ ņåīņĢäņŚÉņä£ ļŗżņ¢æņä▒ ņ¦ĆĒæ£ņØĖ Shannon indexņÖĆ Simpson indexĻ░Ć ņ£Āņé¼ĒĢ©ņØä ļ│┤ņśĆļŗż. ļŗżļ¦ī, richnessļź╝ ļéśĒāĆļé┤ļŖö Chao1Ļ│╝ abundance-based coverage estimatorļŖö ņĀ£ĻĘĀ ņ╣śļŻī ņĀäņŚÉ ļ╣äĒĢ┤ ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ņāüņŖ╣ĒĢśĻĖ░ļŖö ĒĢśņśĆņ£╝ļéś, Ļ▒┤Ļ░ĢĒĢ£ ņåīņĢäņŚÉ ļ╣äĒĢ┤ņä£ļŖö ņ£ĀņØśĒĢśĻ▓ī ļé«ņĢä ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ░ÉņŚ╝ ņĀäņØś richnessņŚÉ ļÅäļŗ¼ĒĢśņ¦ĆļŖö ļ¬╗ĒĢśņśĆļŗż. ļŗżļ¦ī, ņØ┤ ņŚ░ĻĄ¼ņŚÉņä£ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻīļź╝ ļ░øņØĆ ĒÖśņ×ÉņØś ļŗżņłśļŖö ņŗŁņØ┤ņ¦ĆņןĻČżņ¢æņØ┤ ņ׳ņŚłļŖöļŹ░, ņŗŁņØ┤ņ¦ĆņןĻČżņ¢æ ĒÖśņ×ÉņŚÉņä£ ņ£äņĢö ņ£äĒŚśņØ┤ Ļ░ÉņåīĒĢ£ļŗżļŖö ņĀÉņØä Ļ░ÉņĢłĒĢĀ ļĢī, ļ│Ė ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ļź╝ ĒåĀļīĆļĪ£ ņ£äņĢö ļ░£ņāØĻ│╝ ņŚ░Ļ┤Ć ņ׳ļŖö ļ░ĢĒģīļ”¼ņĢäļź╝ ņČöļĪĀĒĢśĻĖ░ņŚÉļŖö ĒĢ£Ļ│äĻ░Ć ņ׳ļŗż[20].
2020ļģä Guo ļō▒[15]ņØĆ ņ┤Ø 58ļ¬ģņØś ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ░ÉņŚ╝ ĒÖśņ×ÉņŚÉ ļīĆĒĢ┤ ņĀ£ĻĘĀ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢśņśĆņ£╝ļ®░, ņĀ£ĻĘĀ ņ╣śļŻī ņä▒Ļ│Ą ĒÖśņ×ÉņØś ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØä ņĀ£ĻĘĀ ņ╣śļŻī ņŗżĒī© ĒÖśņ×ÉņÖĆ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ļ»ĖĻ░ÉņŚ╝ņ×ÉņØś ļ»ĖņāØļ¼╝ĻĄ░ņ¦æĻ│╝ ļ╣äĻĄÉĒĢśņśĆļŗż. ņØ┤ņĀäņØś ļŗżļźĖ ņŚ░ĻĄ¼ņÖĆ ļ¦łņ░¼Ļ░Ćņ¦ĆļĪ£, ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ░ÉņŚ╝ ĒÖśņ×ÉņŚÉņä£ ļé«ņĢäņĀĖ ņ׳ļŖö ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļŗżņ¢æņä▒ņØ┤, ņĀ£ĻĘĀ ņ╣śļŻī ņä▒Ļ│Ą ņŗ£ ņ”ØĻ░ĆĒĢśļŖö Ļ▓āņØä ĒÖĢņØĖĒĢśņśĆļŗż. ņĀ£ĻĘĀ ņ╣śļŻī ņä▒Ļ│Ą ņŗ£ ļŗżņ¢æņä▒ņØĆ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ļ»ĖĻ░ÉņŚ╝ņ×ÉņØś ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æĻ│╝ ļ╣äņŖĘĒĢ£ ņłśņżĆņ£╝ļĪ£ ļ│ĄņøÉļÉśņŚłņ£╝ļ®░, ņĀ£ĻĘĀ ņ╣śļŻī ņŗżĒī© ņŗ£ņŚÉļŖö ņĀ£ĻĘĀ ņ╣śļŻīļź╝ ņŗ£Ē¢ēļ░øĻĖ░ ņĀäĻ│╝ ļ╣äņŖĘĒĢ£ ņĀĢļÅäņØś ļŗżņ¢æņä▒ņØä ļ│┤ņśĆļŗż. ņĀ£ĻĘĀ ņ╣śļŻī ņä▒Ļ│Ą ņŗ£ ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņŚÉļŖö Staphylococcus, Corynebacterium, Fusobacterium, Bacteroides, Streptophyta, Prevotella, Gemella, Porphyromonas, Alloprevotella, Veillonella, Neisseria, Streptococcus, Rothia, HaemophilusņØś ĒÆŹļČĆļÅäĻ░Ć ņ”ØĻ░ĆĒĢśņśĆļŗż. ĻĘĖļ¤¼ļéś ņŻ╝ņä▒ļČä ļČäņäØ(principle component analysis)ņØä ĒåĄĒĢ┤ ņĀäņ▓┤ņĀüņØĖ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æ ņĪ░ņä▒ņØä ļ╣äĻĄÉĒĢśņśĆņØä ļĢīļŖö ņĀ£ĻĘĀ ņ╣śļŻī ņä▒Ļ│Ą ĒÖśņ×ÉņØś ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØ┤ ņĀ£ĻĘĀ ņ╣śļŻī ņĀä ļ»ĖņāØļ¼╝ĻĄ░ņ¦æĻ│╝ ņ░©ņØ┤Ļ░Ć ņ׳ņŚłņ¦Ćļ¦ī, ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ļ»ĖĻ░ÉņŚ╝ņ×ÉņØś ļ»ĖņāØļ¼╝ĻĄ░ņ¦æĻ│╝ ļ╣äĻĄÉĒĢ┤ļÅä ņ░©ņØ┤Ļ░Ć ņ׳ņŚłļŗż. ņĀĆņ×ÉļōżņØĆ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØ┤ ļ│ĄņøÉļÉĀ ņłś ņ׳ņØīņØä ņŻ╝ļĪ£ Ļ░ĢņĪ░ĒĢśĻĖ░ļŖö ĒĢśņśĆņ£╝ļéś, ņĀ£ĻĘĀ ņ╣śļŻīļ¦īņ£╝ļĪ£ ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØ┤ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ░ÉņŚ╝ ņĀäĻ│╝ Ļ░ÖņØ┤ ņÖäņĀäĒ׳ ņĀĢņāüĒÖö ļÉśļŖöĻ░ĆņŚÉ ļīĆĒĢ┤ņä£ļŖö ņØśļ¼ĖņØ┤ ļé©ļŖöļŗż.
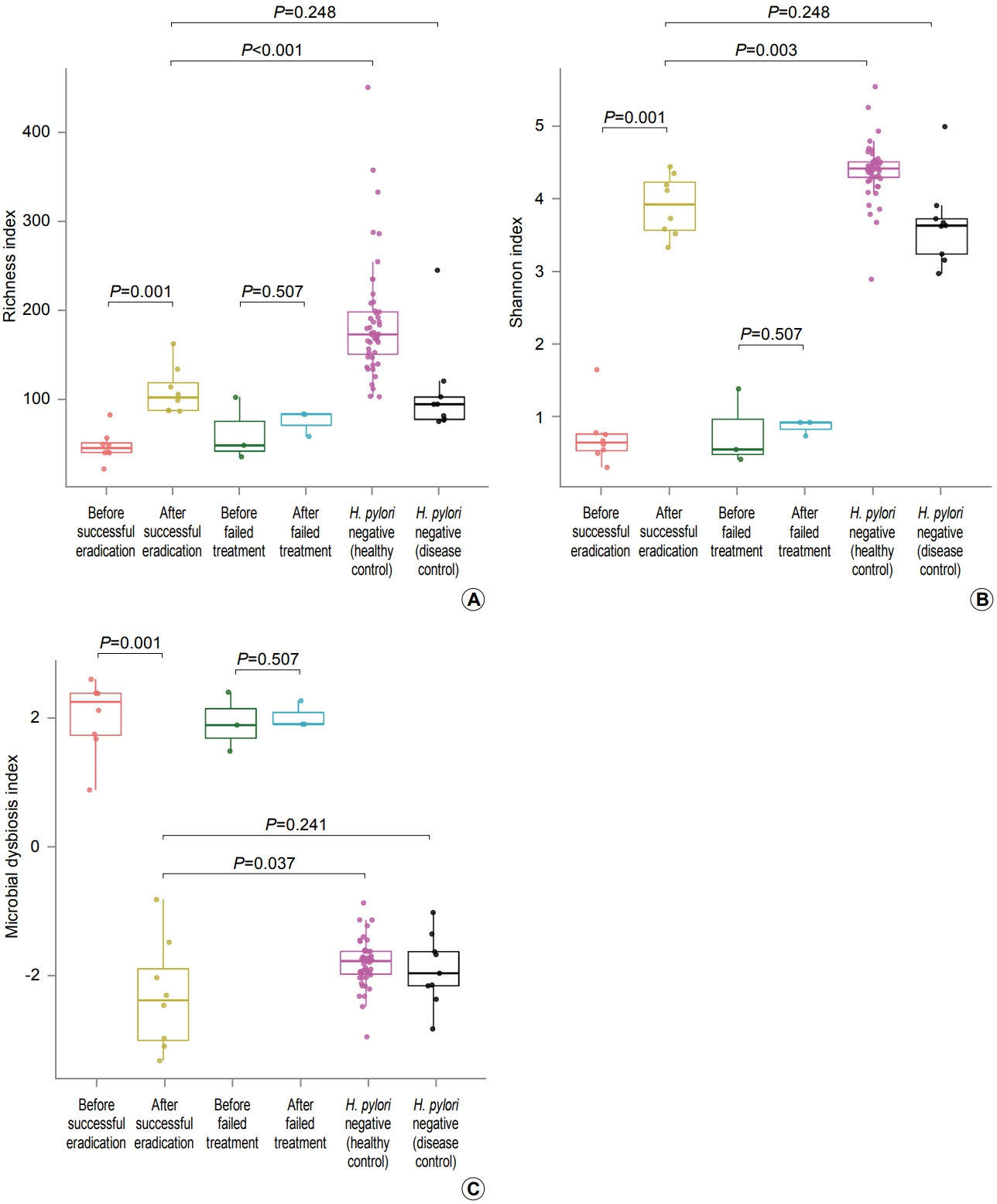
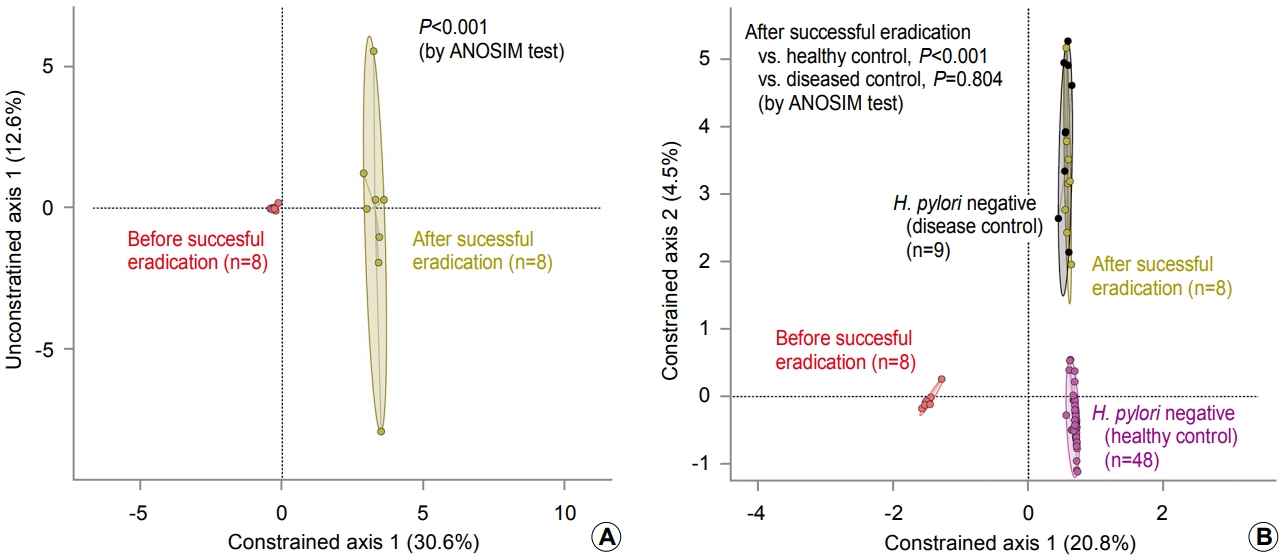
Guo ļō▒[15]ņØś ņŚ░ĻĄ¼ņŚÉņä£ ļ│┤ņŚ¼ņżĆ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻīņŚÉ ļö░ļźĖ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æ ļŗżņ¢æņä▒ņØś ļ│ĄņøÉņØĆ ļ╣äĻĄÉĻĄ░ņØĖ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ļ»ĖĻ░ÉņŚ╝ņ×ÉĻĄ░ņŚÉ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ░ÉņŚ╝ņØ┤ ņŚåņŚłļŹś Ļ▒┤Ļ░ĢņØĖĻ│╝ ņ£äņČĢņä▒ ņ£äņŚ╝ ļ░Å ņןņāüĒö╝ĒÖöņāØņØ┤ ņ¦äĒ¢ēļÉśņ¢┤ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ░ÉņŚ╝ņØ┤ ņåīņŗżļÉ£ Ļ│╝Ļ▒░ Ļ░ÉņŚ╝ņ×ÉĻ░Ć ĒĢ©Ļ╗ś ĒżĒĢ©ļÉśņŚłĻĖ░ ļĢīļ¼ĖņØ╝ Ļ░ĆļŖźņä▒ņØ┤ ņ׳ļŗż. ņØ┤ņŚÉ, ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ļ»ĖĻ░ÉņŚ╝ņ×Éļź╝ Ļ▒┤Ļ░ĢņØĖĻ│╝ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ│╝Ļ▒░ Ļ░ÉņŚ╝ņ×ÉļĪ£ ļČäļ”¼ĒĢśņŚ¼ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī ĒÖśņ×ÉņÖĆ ļ╣äĻĄÉĒĢśĻĖ░ ņ£äĒĢ┤, Guo ļō▒[15]ņØ┤ ņŗ£Ē¢ēĒĢ£ ļČäņäØņØä Park ļō▒[13]ņØś ņŚ░ĻĄ¼ ļŹ░ņØ┤Ēä░ļź╝ ņØ┤ņÜ®ĒĢ┤ ņ×¼ĒśäĒĢ┤ ļ│┤ņĢśļŗż(Fig. 1, 2). Guo ļō▒[15]ņØś ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ņÖĆ ļ¦łņ░¼Ļ░Ćņ¦ĆļĪ£ ņĀ£ĻĘĀ ņ╣śļŻī ņŗżĒī© ņŗ£ richness indexņÖĆ Shannon indexĻ░Ć ņĀ£ĻĘĀ ņ╣śļŻī ņĀäņØś ņłśņ╣śņÖĆ ļ╣äņŖĘĒĢ£ ņłśņżĆņŚÉ ļ©Ėļ¼╝ļ¤¼ ņ׳ļŖö Ļ▓āņŚÉ ļ╣äĒĢ┤, ņĀ£ĻĘĀ ņ╣śļŻī ņä▒Ļ│Ą ņŗ£ņŚÉļŖö ņłśņ╣śĻ░Ć ņāüņŖ╣ĒĢ©ņØä ĒÖĢņØĖĒĢśņśĆļŗż(Fig. 1A, B). ĻĘĖļ¤¼ļéś ņāüņŖ╣ĒĢ£ richness indexņÖĆ Shannon indexļŖö ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ│╝Ļ▒░ Ļ░ÉņŚ╝ņ×ÉņÖĆ ļ╣äņŖĘĒĢ£ ņłśņżĆĻ╣īņ¦Ćļ¦ī ņāüņŖ╣ĒĢśņśĆĻ│Ā, Ļ▒┤Ļ░ĢņØĖņØś ņłśņżĆņŚÉļŖö ļÅäļŗ¼ĒĢśņ¦Ć ļ¬╗ĒĢśņśĆļŗż. Guo ļō▒[15]ņØĆ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī ņä▒Ļ│Ą ņŗ£ ĒÆŹļČĆļÅäĻ░Ć ņ”ØĻ░ĆĒĢśļŖö 17Ļ░£ņØś generaņÖĆ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ņØś ĒÆŹļČĆļÅäļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ļ»ĖņāØļ¼╝ ļČłĻĘĀĒśĢ ņ¦ĆĒæ£(microbial dysbiosis index)ļź╝ ņĀ£ņŗ£ĒĢśņśĆļŖöļŹ░, ņØ┤ ņ¦ĆĒæ£ ņŚŁņŗ£ ņĀ£ĻĘĀ ņ╣śļŻī ņä▒Ļ│Ą ņŗ£ Ļ▒┤Ļ░ĢņØĖļ│┤ļŗżļŖö ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ│╝Ļ▒░ Ļ░ÉņŚ╝ņ×ÉņÖĆ ņ£Āņé¼ĒĢśĻ▓ī ļ│ĆĒÖöĒĢśņśĆļŗż(Fig. 1C). ļśÉĒĢ£, ņŻ╝ņä▒ļČä ļČäņäØ Ļ▓░Ļ│╝ņŚÉņä£ļÅä ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī ņä▒Ļ│Ą ņŗ£ ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ņĪ░ņä▒ņØĆ Ļ▒┤Ļ░ĢņØĖļ│┤ļŗżļŖö ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ│╝Ļ▒░ Ļ░ÉņŚ╝ņ×ÉņÖĆ ļ╣äņŖĘĒĢśņśĆļŗż(Fig. 2).
ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļ│ĆĒÖöļź╝ ļČäņäØĒĢ£ Ēśäņ×¼Ļ╣īņ¦ĆņØś ļ¬©ļōĀ ņŚ░ĻĄ¼Ļ░Ć ņØ╝Ļ┤ĆļÉśĻ▓ī ļ│┤ņŚ¼ņŻ╝ļŖö ņåīĻ▓¼ņØĆ ņĀ£ĻĘĀ ņ╣śļŻī ņä▒Ļ│Ą ņŗ£ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņÖĖ ļŗżļźĖ ņŚ¼ļ¤¼ ļ░ĢĒģīļ”¼ņĢäņØś ĒÆŹļČĆļÅäĻ░Ć ņ”ØĻ░ĆĒĢśĻ│Ā ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļŗżņ¢æņä▒ņØ┤ ņ”ØĻ░ĆĒĢ£ļŗżļŖö ņĀÉņØ┤ļŗż(Fig. 3). ĻĘĖļ¤¼ļéś ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ņ¢┤ļ¢ż ļ░ĢĒģīļ”¼ņĢä ļČäļźśĻĄ░ņØ┤ ņāüļīĆņĀüņ£╝ļĪ£ ļåÆņØĆ ļ╣äņ£©ļĪ£ ņ”ØĻ░ĆĒĢśļŖöņ¦ĆļŖö ņŚ░ĻĄ¼ļ¦łļŗż ņ░©ņØ┤Ļ░Ć ņ׳Ļ│Ā, ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ņĪ░ņä▒Ļ│╝ ļŗżņ¢æņä▒ņØ┤ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ░ÉņŚ╝ ņØ┤ņĀäĻ│╝ Ļ░ÖņØ┤ ņÖäņĀäĒ׳ ļ│ĄņøÉļÉśļŖöĻ░ĆņŚÉ ļīĆĒĢ┤ņä£ļŖö ņŚ░ĻĄ¼ļ¦łļŗż ņ░©ņØ┤Ļ░Ć ņ׳ļŗż. ņØ┤ļŖö ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ņĪ░ņä▒ņŚÉ ņŚ¼ļ¤¼ ņ¦ĆņŚŁņĀü, ĒÖśĻ▓ĮņĀü ņØĖņ×ÉĻ░Ć Ļ┤ĆņŚ¼ĒĢ©ņØĆ ļ¼╝ļĪĀņØ┤Ļ│Ā, ņŚ░ĻĄ¼ ļīĆņāüņ×ÉņØś ņ£ä ļé┤ ņ¦łļ│æ ņāüĒā£(ņ£äņŚ╝, ņ£äņČĢņä▒ ņ£äņŚ╝, ņןņāüĒö╝ĒÖöņāØ)Ļ░Ć ņŚ░ĻĄ¼ļ¦łļŗż ņ░©ņØ┤Ļ░Ć ņ׳ĻĖ░ ļĢīļ¼Ėņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż[8,21]. Ļ░Ćņן ņĄ£ĻĘ╝ņŚÉ ļ░£Ēæ£ļÉ£ 2020ļģä Sung ļō▒[6]ņØś ņŚ░ĻĄ¼ļŖö 102ļ¬ģņØś ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ░ÉņŚ╝ņ×ÉņŚÉĻ▓ī ņĀ£ĻĘĀ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢśĻ│Ā 1ļģä Ēøä ņ£äņŚ╝ņØ┤ ņ¦ĆņåŹļÉśĻ▒░ļéś, ņ£äņČĢņä▒ ņ£äņŚ╝ Ēś╣ņØĆ ņןņāüĒö╝ĒÖöņāØņØ┤ ņāłļĪ£ ļ░£ņāØĒĢ£ ĒÖśņ×ÉņØś ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ĒŖ╣ņä▒ņØä ļČäņäØĒĢśņśĆļŗż. ĒØźļ»ĖļĪŁĻ▓īļÅä, ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻīĻ░Ć ņä▒Ļ│ĄĒĢśņśĆļŹöļØ╝ļÅä ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ņĪ░ņä▒ņØĆ ĒÖśņ×É Ļ░äņŚÉ ņ░©ņØ┤Ļ░Ć ņ׳ņŚłļŖöļŹ░, 1ļģä Ēøä ņ£äņŚ╝ņØ┤ ņ¦ĆņåŹļÉśņŚłļŹś ĒÖśņ×ÉņŚÉņä£ļŖö ĻĘĖļĀćņ¦Ć ņĢŖņØĆ ĒÖśņ×Éļ│┤ļŗż Acinetobacter lwoffii, Streptococcus anginosus, RalstoniaņØś ĒÆŹļČĆļÅäĻ░Ć ņ”ØĻ░ĆĒĢśņśĆĻ│Ā, ņ£äņČĢņä▒ ņ£äņŚ╝ņØ┤ ņāłļĪ£ ļ░£ņāØĒĢ£ ĒÖśņ×ÉņŚÉņä£ļŖö ĻĘĖļĀćņ¦Ć ņĢŖņØĆ ĒÖśņ×Éļ│┤ļŗż Granulicatella, Streptococcus, Rothia, LeptotrichiaņØś ĒÆŹļČĆļÅäĻ░Ć ņ”ØĻ░ĆĒĢśņśĆņ£╝ļ®░, ņןņāüĒö╝ĒÖöņāØņØ┤ ņāłļĪ£ ļ░£ņāØĒĢ£ ĒÖśņ×ÉņŚÉņä£ļŖö ĻĘĖļĀćņ¦Ć ņĢŖņØĆ ĒÖśņ×Éļ│┤ļŗż Mesorhizobium, CupriavidusņØś ĒÆŹļČĆļÅäĻ░Ć ņ”ØĻ░ĆĒĢśņśĆļŗż. Sung ļō▒[6]ņØĆ ņØ┤ļōż ļ»ĖņāØļ¼╝ ļČäļźśĻĄ░ņØ┤ ņ×Āņ×¼ņĀüņ£╝ļĪ£ ņ£äņĢö ļ░£ļ│æņŚÉ ĻĖ░ņŚ¼ĒĢśļŖö ņ£ä ļé┤ ļ»ĖņāØļ¼╝ņØ┤Ļ│Ā ņ£äņĢö ņśłļ░®ņØś ĒāĆĻ▓¤ņØ┤ ļÉĀ ņłśļÅä ņ׳ņØīņØä Ļ░ĢņĪ░ĒĢśņśĆļŗż. ļ¼╝ļĪĀ, ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī 1ļģä Ēøä ņןņāüĒö╝ĒÖöņāØņØ┤ ņāłļĪ£ņØ┤ ļ░£ņāØĒĢ£ ĒÖśņ×ÉņŚÉņä£ ļ│┤ļŗż ļ¦ÄņØ┤ ļ░£Ļ▓¼ļÉśļŖö Mesorhizobium Ēś╣ņØĆ CupriavidusņÖĆ Ļ░ÖņØĆ ļ░ĢĒģīļ”¼ņĢäĻ░Ć ņŗżņĀ£ļĪ£ ņןņāüĒö╝ĒÖöņāØņØä ņ£Āļ░£ĒĢ£ ļ»ĖņāØļ¼╝ņØĖņ¦Ć, ņĢäļŗłļ®┤ ņןņāüĒö╝ĒÖöņāØņØ┤ ļ░£ņāØĒĢśņśĆĻĖ░ ļĢīļ¼ĖņŚÉ ņØ┤ņ░©ņĀüņ£╝ļĪ£ ņ”ØņŗØļÉ£ ļ»ĖņāØļ¼╝ņØĖņ¦Ć ĒīÉļŗ©ĒĢśĻĖ░ļŖö ņĢäņ¦ü ņØ┤ļź┤ļéś, ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻīļź╝ ļ░øņØĆ ļ¬©ļōĀ ĒÖśņ×ÉņŚÉņä£ ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØ┤ Ļ▒┤Ļ░ĢņØĖĻ│╝ Ļ░ÖņØĆ ņłśņżĆņ£╝ļĪ£ ļ│ĄņøÉļÉśļŖö Ļ▓āņØĆ ņĢäļŗī Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż.
3. ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻīņŚÉ ļö░ļźĖ ņ£ä ļé┤ ļ®öĒāĆņ£ĀņĀäņ▓┤(metagenome)ņØś ĻĖ░ļŖź ļ│ĆĒÖö
ņ¦ĆĻĖłĻ╣īņ¦Ć ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļ│ĆĒÖöļź╝ ļ│Ė ņŚ░ĻĄ¼ļŖö ļīĆļČĆļČä 16S rRNA ņ£ĀņĀäņ×É ņŗ£ĒĆĆņŗ▒ņØä ņØ┤ņÜ®ĒĢśņŚ¼ ņ¦äĒ¢ēļÉśņŚłļŗż. 16S rRNA ņ£ĀņĀäņ×É ņŗ£ĒĆĆņŗ▒ņØä ņØ┤ņÜ®ĒĢ£ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æ ņŚ░ĻĄ¼ļŖö ļ░ĢĒģīļ”¼ņĢäņØś 16S rRNA ņ£ĀņĀäņ×É ņŚ╝ĻĖ░ ņä£ņŚ┤ļ¦īņØä ļČäņäØĒĢśņŚ¼ ņ¢┤ļ¢ż ļČäļźśĻĄ░ņØś ļ░ĢĒģīļ”¼ņĢäĻ░Ć ņ¢┤ļŖÉ ņĀĢļÅä ņĪ┤ņ×¼ĒĢśļŖöĻ░Ćļź╝ ņĢīņĢäļé┤ļŖö Ļ▓āņØ┤ļ®░ ļ®öĒāĆņ£ĀņĀäņ▓┤ņØś ļ¬©ļōĀ ņ£ĀņĀäņ×É ņŚ╝ĻĖ░ ņä£ņŚ┤ņØä ņ¦üņĀæ ļČäņäØĒĢśļŖö Ļ▓āņØ┤ ņĢäļŗłĻĖ░ ļĢīļ¼ĖņŚÉ, ļ®öĒāĆņ£ĀņĀäņ▓┤ņØś ĻĖ░ļŖźņØä ņ¦üņĀæņĀüņ£╝ļĪ£ ĒīīņĢģĒĢĀ ņłśļŖö ņŚåļŗż. ĻĘĖļ¤¼ļéś ĒåĀņ¢æņØ┤ļéś ņŗØļ¼╝ ļō▒ņŚÉ ņĪ┤ņ×¼ĒĢśļŖö ļ®öĒāĆņ£ĀņĀäņ▓┤ņÖĆļŖö ļŗ¼ļ”¼ ņé¼ļ×īņØś ņן ļé┤ņŚÉ ņĪ┤ņ×¼ĒĢśļŖö ļ®öĒāĆņ£ĀņĀäņ▓┤ļŖö ļīĆļČĆļČä ĻĘĖ ĻĖ░ļŖźņØ┤ ņĢīļĀżņĀĖ ņ׳ĻĖ░ ļĢīļ¼ĖņŚÉ, ņé¼ļ×īņŚÉ ļīĆĒĢ£ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æ ņŚ░ĻĄ¼ņØś Ļ▓ĮņÜ░ņŚÉļŖö 16S rRNA ņŗ£ĒĆĆņŗ▒ņØä ĒåĄĒĢ┤ ņĢīņĢäļéĖ operational taxonomic unitņŚÉ ļīĆĒĢ£ ņĀĢļ│┤ļ¦īņØä Ļ░¢Ļ│Ā ļ®öĒāĆņ£ĀņĀäņ▓┤ņØś ĻĖ░ļŖźņØä ļ╣äĻĄÉņĀü ņĀĢĒÖĢĒ׳ ņČöļĪĀĒĢĀ ņłś ņ׳ļŗż[22,23].
Table 1ņŚÉ ņĀ£ņŗ£ļÉ£ 8Ļ▒┤ņØś ņŚ░ĻĄ¼ ņżæ 5Ļ▒┤ņØś ņŚ░ĻĄ¼ņŚÉņä£ ļ®öĒāĆņ£ĀņĀäņ▓┤ ĻĖ░ļŖźņØä ļČäņäØĒĢśņśĆĻ│Ā, ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻīņŚÉ ļö░ļźĖ ļ®öĒāĆņ£ĀņĀäņ▓┤ņØś ĻĖ░ļŖź ļ│ĆĒÖöļŖö 4Ļ▒┤ņØś ņŚ░ĻĄ¼ņŚÉņä£ ļ│┤Ļ│ĀļÉśņŚłļŗż[6,12,13,15]. He ļō▒[12]ņØĆ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī ņĀäņŚÉ ļ╣äĒĢ┤ ņĀ£ĻĘĀ ņ╣śļŻī Ēøä lipopolysaccharide biosynthesis, lipopolysaccharide biosynthesis proteins, bacterial motility proteins, bacterial chemotaxis Ļ┤ĆļĀ© ĻĖ░ļŖźņØ┤ Ļ░ÉņåīĒĢśĻ│Ā, glycolysis/gluconeogenesis, glycine, serine, threonine metabolism, pentose phosphate pathway Ļ┤ĆļĀ© ĻĖ░ļŖźņØĆ ņ”ØĻ░ĆĒĢ©ņØä ļ│┤Ļ│ĀĒĢśņśĆļŗż. Park ļō▒[13]ņØś ņŚ░ĻĄ¼ņŚÉņä£ļŖö Ļ▒┤Ļ░ĢņØĖņŚÉ ļ╣äĒĢ┤ ņןņāüĒö╝ĒÖöņāØ ĒÖśņ×ÉņŚÉņä£ ņ”ØĻ░ĆĒĢ£ ļŗżņ¢æĒĢ£ ļ®öĒāĆņ£ĀņĀäņ▓┤ ņ£ĀņĀäņ×Éļź╝ ļ│┤Ļ│ĀĒĢśņśĆļŖöļŹ░ ņØ┤ ņżæ type IV secretion system (T4SS) ļŗ©ļ░▒ņ¦ł ņĮöļö® ņ£ĀņĀäņ×ÉĻ░Ć ņ”ØĻ░ĆĒĢ┤ ņ׳ņŚłĻ│Ā, ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ░ÉņŚ╝ ņ£äņŚ╝ ĒÖśņ×ÉņŚÉņä£ ņĀ£ĻĘĀ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢ£ ĒøäņŚÉļÅä ļ®öĒāĆņ£ĀņĀäņ▓┤ņŚÉ T4SS ļŗ©ļ░▒ņ¦ł ņĮöļö® ņ£ĀņĀäņ×ÉĻ░Ć ņ”ØĻ░ĆĒĢśņśĆņØīņØä ļ│┤Ļ│ĀĒĢśņśĆļŗż. T4SS ļŗ©ļ░▒ņ¦łņØĆ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ņØś CagA ļŗ©ļ░▒ņ¦łņØ┤ ņé¼ļ×īņØś ņ£ä ņāüĒö╝ņäĖĒżļĪ£ ņĀäļŗ¼ļÉśļŖöļŹ░ ĒĢäņłśņĀüņØĖ ļŗ©ļ░▒ņ¦łļĪ£, ņןņāüĒö╝ĒÖöņāØ ĒÖśņ×ÉņØś ļ®öĒāĆņ£ĀņĀäņ▓┤ņŚÉņä£ ņ”ØĻ░ĆĒĢśļŖö T4SS ļŗ©ļ░▒ņ¦ł ņĮöļö® ņ£ĀņĀäņ×ÉļŖö ņ£äņĢöņØś ļ░£ļ│æ ņ£äĒŚś ņ”ØĻ░ĆņÖĆ Ļ┤ĆļĀ©ņØ┤ ņ׳ņØä Ļ░ĆļŖźņä▒ņØ┤ ņĀ£ņŗ£ļÉśņŚłļŗż[13]. ļśÉĒĢ£, ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢĀ Ļ▓ĮņÜ░ ļ®öĒāĆņ£ĀņĀäņ▓┤ņŚÉ T4SS ļŗ©ļ░▒ņ¦ł ņĮöļö® ņ£ĀņĀäņ×ÉĻ░Ć ņ”ØĻ░ĆĒĢ©ņŚÉļÅä ļČłĻĄ¼ĒĢśĻ│Ā ņ£äņĢöņØś ļ░£ļ│æ ņ£äĒŚśņØ┤ Ļ░ÉņåīĒĢ£ļŗżļŖö ņĀÉņØĆ ņ£äņĢöņØś ļ░£ņāØņŚÉ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņÖĖ ļ░ĢĒģīļ”¼ņĢäņØś ņĪ┤ņ×¼ļÅä ņżæņÜöĒĢĀ ņłś ņ׳ņ¦Ćļ¦ī ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņ×Éņ▓┤Ļ░Ć ļ│┤ļŗż ņżæņÜöĒĢ£ ņØĖņ×Éņ×äņØä ņŗ£ņé¼ĒĢ£ļŗż[13].
Guo ļō▒[15]ņØĆ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ļ®öĒāĆņ£ĀņĀäņ▓┤ņŚÉ ļŗ©ļ░▒ņ¦łņØś ņåīĒÖöņÖĆ ĒØĪņłś, glucosaminoglycanĻ│╝ ĻĖ░ĒāĆ glycanņØś ļČäĒĢ┤, ņ£äņé░ ļČäļ╣ä ļ░Å ĒāäņłśĒÖöļ¼╝ņØś ņåīĒÖöņÖĆ ĒØĪņłś Ļ┤ĆļĀ© ĻĖ░ļŖźņØ┤ ņ”ØĻ░ĆĒĢśĻ│Ā, ĒÄĖļ¬© ļČĆņåŹņןņ╣ś(flagellar assembly), ņäĖĻĘĀņØś ĒÖöĒĢÖņŻ╝ņä▒(chemotaxis) ļ░Å ņäĖĻĘĀļČäļ╣äņ▓┤Ļ│ä Ļ┤ĆļĀ© ĻĖ░ļŖźņØ┤ ņżäņ¢┤ļō”ņØä ļ│┤ņŚ¼ņŻ╝ņŚłļŗż. Sung ļō▒[6]ņØś ņŚ░ĻĄ¼ņŚÉņä£ļŖö ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī 1ļģä Ļ▓ĮĻ│╝ Ēøä, ņןņāüĒö╝ĒÖöņāØņØ┤ ļ░£ņāØĒĢśņ¦Ć ņĢŖņØĆ ĒÖśņ×ÉņØś ļ®öĒāĆņ£ĀņĀäņ▓┤ņŚÉ ļ╣äĒĢ┤ ņןņāüĒö╝ĒÖöņāØ ņØ┤ ņāłļĪ£ ļ░£ņāØĒĢ£ ĒÖśņ×ÉņØś ļ®öĒāĆņ£ĀņĀäņ▓┤ņŚÉņä£ ņĢäļ»ĖļģĖņé░ ļ░Å inositol phosphate ļīĆņé¼ Ļ┤ĆļĀ© ĻĖ░ļŖź ņ£ĀņĀäņ×ÉņÖĆ T4SS ļŗ©ļ░▒ņ¦ł ņĮöļö® ņ£ĀņĀäņ×ÉĻ░Ć ņ”ØĻ░ĆĒĢ©ņØä ĒÖĢņØĖĒĢśņśĆļŗż.
ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ļŗżņ¢æĒĢ£ ļ░ĢĒģīļ”¼ņĢä ļČäļźśĻĄ░ņØś ĒÆŹļČĆļÅäĻ░Ć ņ”ØĻ░ĆĒĢśĻ│Ā, ĻĘĖņŚÉ ļö░ļØ╝ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ļ®öĒāĆņ£ĀņĀäņ▓┤ņØś ĻĖ░ļŖź ņŚŁņŗ£ ļ¦ÄņØĆ ļ│ĆĒÖöļź╝ ļ│┤ņ×äņØ┤ ņŚ¼ļ¤¼ ņŚ░ĻĄ¼ņŚÉņä£ ĒÖĢņØĖļÉśņŚłļŗż. ĻĘĖļ¤¼ļéś ņĢ×ņä£ ņé┤ĒÄ┤ļ│Ė ļ░öņÖĆ Ļ░ÖņØ┤ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ņ”ØĻ░ĆĒĢśļŖö ļ░ĢĒģīļ”¼ņĢä ļČäļźśĻĄ░ņØĆ ņŚ░ĻĄ¼ļ¦łļŗż ņ░©ņØ┤ļź╝ ļ│┤ņØ┤ļ®░, ļ®öĒāĆņ£ĀņĀäņ▓┤ņØś ĻĖ░ļŖź ļ│ĆĒÖö ņŚŁņŗ£ ņŚ░ĻĄ¼ņŚÉ ļö░ļØ╝ ņ░©ņØ┤Ļ░Ć ņ׳ļŗż. ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ļ│ĆĒÖöĒĢśļŖö ļ®öĒāĆņ£ĀņĀäņ▓┤ņØś ĻĖ░ļŖźņØä ĒāÉņāēĒĢśļŖö Ļ▓āņØĆ ņ£äņĢöņØś ļ░£ļ│æ ĻĖ░ņĀä ĻĘ£ļ¬ģņŚÉ ļÅäņøĆņØä ņżä ņłśļŖö ņ׳ņ£╝ļéś, ņĢäņ¦üĻ╣īņ¦Ć ļ®öĒāĆņ£ĀņĀäņ▓┤ņØś ĻĖ░ļŖźņØ┤ ņ£äņĢö ļ░£ļ│æņŚÉ ņ¦üņĀæņĀüņ£╝ļĪ£ ļ»Ėņ╣śļŖö ņśüĒ¢źņØ┤ ĒÖĢņŗżĒ׳ ļ░ØĒśĆņ¦Ćņ¦ĆļŖö ņĢŖņĢśļŗż. ĒĢ£ Ļ░Ćņ¦Ć ņżæņÜöĒĢśĻ▓ī ĻĖ░ņ¢ĄĒĢĀ Ļ▓āņØĆ ņןņāüĒö╝ĒÖöņāØ ĒÖśņ×ÉņŚÉņä£ ņ”ØĻ░ĆĒĢśļŖö ļ®öĒāĆņ£ĀņĀäņ▓┤ ĻĖ░ļŖźņØ┤ļéś, Ēś╣ņØĆ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī Ēøä Ļ░ÉņåīĒĢśļŖö ļ®öĒāĆņ£ĀņĀäņ▓┤ ĻĖ░ļŖźņØ┤ ļ¬©ļæÉ ņ£äņĢöņØś ļ░£ļ│æņŚÉ ņśüĒ¢źņØä ļ»Ėņ╣śļŖö Ļ▓āņØĆ ņĢäļŗłļØ╝ļŖö ņĀÉņØ┤ļŗż. ļ░ĢĒģīļ”¼ņĢäņØś ņ£ĀņĀäņ▓┤ ļīĆļČĆļČäņØĆ ļ░ĢĒģīļ”¼ņĢä ņ×ÉņŗĀņØś ņāØņĪ┤Ļ│╝ ņ”ØņŗØņŚÉ ĒĢäņÜöĒĢ£ Ļ▓āņØ┤ņ¦Ć, ņłÖņŻ╝ņØś ņ£äņĢö ļ░£ļ│æņØä ņ£äĒĢ£ ļ¬®ņĀüņ£╝ļĪ£ ņĪ┤ņ×¼ĒĢśļŖö Ļ▓āņØĆ ņĢäļŗłĻĖ░ ļĢīļ¼ĖņØ┤ļŗż. ļö░ļØ╝ņä£, ņ£äņĢöņØś ļ░£ļ│æ ĻĖ░ņĀäņØä ĻĘ£ļ¬ģĒĢśĻ│Āņ×É ĒĢĀ ļĢī, ļŗ©ņł£Ē׳ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī ņĀä/Ēøä ļ│ĆĒÖöļ¤ēņØ┤ Ēü░ ļ®öĒāĆņ£ĀņĀäņ▓┤ ĻĖ░ļŖźņŚÉļ¦ī ņ┤łņĀÉņØä ļ¦×ņČöņ¢┤ ĒśäņāüņØä ņØ┤ĒĢ┤ĒĢśĻĖ░ļ│┤ļŗżļŖö, ņĀ£ĻĘĀ ņ╣śļŻī ņĀä/Ēøä ļ│ĆĒÖöļ¤ēņØ┤ Ēü¼ņ¦Ć ņĢŖļŹöļØ╝ļÅä ņ£äņĢö ļ░£ļ│æĻ│╝ ņŚ░Ļ┤Ćņä▒ņØ┤ ņ׳ņØä ņłś ņ׳ļŖö ņ£ĀņĀäņ×É ĻĖ░ļŖźņØä ņäĀļ│äĒĢśņŚ¼ ļČäņäØĒĢśļĀżļŖö ļģĖļĀźņØ┤ ĒĢäņÜöĒĢśļŗż.
Ļ▓░ ļĪĀ
ņ¦ĆĻĖłĻ╣īņ¦Ć ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻī ņĀä/Ēøä ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļ│ĆĒÖö ņ¢æņāüņŚÉ ļīĆĒĢ┤ ņé┤ĒÄ┤ļ│┤ņĢśļŗż. ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ░ÉņŚ╝ ĒÖśņ×ÉņØś ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņŚÉļŖö ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼Ļ░Ć ļ¦żņÜ░ ļåÆņØĆ ļ╣äņżæņØä ņ░©ņ¦ĆĒĢśĻ│Ā ņ׳Ļ│Ā ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļŗżņ¢æņä▒ņØĆ ļé«ņĢäņĀĖ ņ׳ņ£╝ļ®░, ņĀ£ĻĘĀ ņ╣śļŻī Ēøä ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØś ļŗżņ¢æņä▒ņØĆ ņ”ØĻ░ĆĒĢ£ļŗż. ĻĘĖļ¤¼ļéś ņ£ä ļé┤ ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØ┤ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ ņĀ£ĻĘĀ ņ╣śļŻīļź╝ ĒåĄĒĢ┤ ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ░ÉņŚ╝ ņĀäņ£╝ļĪ£ ņÖäņĀäĒ׳ ļ│ĄņøÉļÉĀ ņłś ņ׳ļŖöĻ░ĆņŚÉ ļīĆĒĢ┤ņä£ļŖö ļģ╝ļ×ĆņØ┤ ņ׳ņ£╝ļ®░, ņĀ£ĻĘĀ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢśņśĆļŹöļØ╝ļÅä ņ£äņČĢņä▒ ņ£äņŚ╝ņØ┤ļéś ņןņāüĒö╝ĒÖöņāØņØ┤ ļ░£ņāØĒĢ£ ĒÖśņ×ÉņØś ļ»ĖņāØļ¼╝ĻĄ░ņ¦æņØĆ ĻĘĖļĀćņ¦Ć ņĢŖņØĆ ĒÖśņ×ÉņØś ļ»ĖņāØļ¼╝ĻĄ░ņ¦æĻ│╝ ņ░©ņØ┤Ļ░Ć ņ׳ļŗż.