ņä£ ļĪĀ
Epstein-Barr virus (EBV)ļŖö Herpes virusņŚÉ ņåŹĒĢśļŖö ņØ┤ņżæ ļéśņäĀĒśĢņØś DNA ļ░öņØ┤ļ¤¼ņŖżņØ┤Ļ│Ā, ĻĄ¼ņØĖļæÉņØś ņāüĒö╝ņäĖĒżņŚÉņä£ ņ”ØņŗØĒĢśļ®┤ņä£ ņŻ╝ļĪ£ ĒāĆņĢĪņØä ĒåĄĒĢ┤ ņĀäĒīīļÉ£ļŗż. ņøÉļ░£ņä▒ Ļ░ÉņŚ╝ņØĆ ņåīņĢäĻĖ░ņŚÉ ļ│äļŗżļźĖ ņ”Øņāü ņŚåņØ┤ ņ¦ĆļéśĻ░ĆĻ│Ā, ņØ┤ĒøäļĪ£ļŖö Bļ”╝ĒöäĻĄ¼ņŚÉ ļ¼┤ņ”ØņāüņØś ņ×Āļ│Ą Ļ░ÉņŚ╝ ĒśĢĒā£ļź╝ ļ│┤ņØ┤ļŖöļŹ░, ņĀä ņäĖĻ│ä ņä▒ņØĖ ņØĖĻĄ¼ņØś 90% ņØ┤ņāüņŚÉņä£ ņ¢æņä▒ Ēśłņ▓Łļ░śņØæņØä ļ│┤ņØ┤ļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[1]. EBV Ļ░ÉņŚ╝ņØś ļæÉ Ļ░Ćņ¦Ć ņŻ╝ Ēæ£ņĀüņäĖĒżļŖö ņ×Āļ│Ą Ļ░ÉņŚ╝ņØä ļéśĒāĆļé┤ļŖö Bļ”╝ĒöäĻĄ¼ņÖĆ ļ░öņØ┤ļ¤¼ņŖż ņ”ØņŗØņØ┤ ņØ╝ņ¢┤ļéśļŖö ņØĖĒøäļæÉņāüĒö╝ņäĖĒżļĪ£ ļ▓äĒéżĒŖĖ ļ”╝Ēöäņóģ(BurkittŌĆÖs lymphoma), ļ╣äĒśĖņ¦ĆĒé© ļ”╝Ēöäņóģ(non-HodgikinŌĆÖs lymphoma), ĒśĖņ¦ĆĒé© ļ”╝Ēöäņóģ(HodgikinŌĆÖs lymphoma), ņØ┤ņŗØĒøä ļ”╝Ēöäņ”ØņŗØņä▒ņ¦łĒÖś(post-transplant lymphoproliferative disorder), ļ╣äņØĖļæÉņĢö(nasopharyngeal carcinoma)Ļ│╝ Ļ░ÖņØĆ ņĢģņä▒ ņóģņ¢æņØä ņ£Āļ░£ĒĢĀ ņłś ņ׳ņ¢┤ International Agency for Research on CancerņŚÉņä£ļŖö EBVļź╝ group-1 carcinogenņ£╝ļĪ£ ļČäļźśĒĢśĻ│Ā ņ׳ļŗż[2].
1990ļģä Burke ļō▒ņØ┤ EBVņÖĆ ņŚ░Ļ┤ĆļÉ£ ņ£äņĢö(EBV-associated gastric carcinoma, EBVaGC)ņØä ņ▓śņØīņ£╝ļĪ£ ļ│┤Ļ│ĀĒĢ£ ņØ┤Ēøä ņØ┤ņŚÉ ļīĆĒĢ£ ņŚ¼ļ¤¼ ņŚ░ĻĄ¼ļōżņØ┤ ņ׳ņŚłļŗż. ņĄ£ĻĘ╝ ļ│┤Ļ│ĀņŚÉ ļö░ļź┤ļ®┤ EBVaGCļŖö EBV ņŚ░Ļ┤Ć ņĢģņä▒ ņóģņ¢æ Ļ░ĆņÜ┤ļŹ░ Ļ░Ćņן ĒØöĒĢśĻ│Ā, ņĀä ņäĖĻ│äņĀüņ£╝ļĪ£ ņŚ░Ļ░ä 75,000-90,000ņśł ņĀĢļÅä ļ░£ņāØĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż. ņØ┤ļŖö ņĀäņ▓┤ ņ£äņĢö ņżæ 10%ļź╝ ņ░©ņ¦ĆĒĢśļ®░, ņÜ░ļ”¼ļéśļØ╝ņŚÉņä£ļŖö ņĀäņ▓┤ ņ£äņĢöņØś 5.6~13%Ļ░Ć EBV Ļ░ÉņŚ╝Ļ│╝ ņŚ░Ļ┤Ćņä▒ņØ┤ ņ׳ļŗżĻ│Ā ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ļŗż[3-5]. EBVaGCļŖö ņ£äņĢöņØś ļČäņ×ÉĒĢÖņĀü ļČäļźśņŚÉ ļö░ļØ╝ ļ│äļÅäņØś ņ£ĀĒśĢņ£╝ļĪ£ ļČäļźśĒĢśĻ│Ā ņ׳ņ£╝ļ®░, ļŗżļźĖ ņ£ĀĒśĢņØś ņ£äņĢöĻ│╝ļŖö ļŗżļźĖ ņ£ĀņĀäņĀü, ņ×äņāüļ│æļ”¼ĒĢÖņĀüņØĖ ĒŖ╣ņä▒ņØä ļ│┤ņØ┤ļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż(Table 1) [3].
ļ│ĖĻ│ĀņŚÉņä£ļŖö EBVaGCņØś ļ│æņØĖĻ│╝ ņ×äņāüļ│æļ”¼ĒĢÖņĀü ĒŖ╣ņ¦ĢņØä Ļ│Āņ░░ĒĢ┤ļ│┤Ļ│Ā ņŗżņĀ£ ņ¦äļŻīņŚÉņä£ ĻĘĖ ņ×äņāüņĀü ņØśņØśņŚÉ ļīĆĒĢ┤ ņĢīņĢäļ│┤Ļ│Āņ×É ĒĢśņśĆļŗż.
ļ│Ė ļĪĀ
1. ļ│æņØĖ
EBVĻ░Ć ņ¢┤ļ¢ż Ļ▓ĮļĪ£ļĪ£ ņ£äņĀÉļ¦ē ņāüĒö╝ņäĖĒżņŚÉ ņ╣©ņ×ģĒĢśļŖöņ¦ĆņŚÉ ļīĆĒĢ┤ņä£ļŖö ņĢäņ¦üļÅä ļČłļČäļ¬ģĒĢśļŗż. ņ£äņĀÉļ¦ē ņāüĒö╝ņäĖĒżņŚÉļŖö CD21 antigen (C3d/EBV-receptor)ņØ┤ ņŚåĻĖ░ ļĢīļ¼ĖņŚÉ ļ░öņØ┤ļ¤¼ņŖżņŚÉ ņØśĒĢ£ ņ£äņĀÉļ¦ē ņāüĒö╝ņäĖĒżļĪ£ņØś ņ¦üņĀæ Ļ░ÉņŚ╝ Ļ░ĆļŖźņä▒ņØĆ ļé«Ļ│Ā, EBVņŚÉ Ļ░ÉņŚ╝ļÉ£ ņ£äņĀÉļ¦ē Ļ│Āņ£ĀņĖĄņØś Bļ”╝ĒöäĻĄ¼ņŚÉ ņØśĒĢśņŚ¼ ņ£äņĀÉļ¦ē ņāüĒö╝ņäĖĒżņÖĆ ņäĖĒż ņ£ĄĒĢ®ņØä ņØ╝ņ£╝ĒéżĻ▒░ļéś EBV-specific IgAļź╝ ļ¦żĻ░£ņ▓┤ļĪ£ ĒĢśņŚ¼ ļ░öņØ┤ļ¤¼ņŖżļź╝ ņ£äņĀÉļ¦ē ņāüĒö╝ņäĖĒżļĪ£ ņĀäļŗ¼ĒĢĀ Ļ▓āņØ┤ļØ╝ļŖö Ļ░ĆņäżņØ┤ ņ£ĀļĀźĒĢśļŗż[6]. ĒĢśņ¦Ćļ¦ī ņĢäņ¦ü ņĢīļĀżņ¦Ćņ¦Ć ņĢŖņØĆ ļ░öņØ┤ļ¤¼ņŖż ņłśņÜ®ņ▓┤ļź╝ ļ¦żĻ░£ļĪ£ ĒĢśņŚ¼ EBVĻ░Ć ņ£äņĀÉļ¦ē ņāüĒö╝ņäĖĒżļĪ£ ņ¦üņĀæ ņ╣©Ēł¼ĒĢĀ ņłś ņ׳ļŗżļŖö ņØśĻ▓¼ļÅä ņ׳ļŗż[6]. ĒĢ£ĒÄĖ EBV Ļ░ÉņŚ╝ņØĆ ņĢöĒÖö Ļ│╝ņĀĢ(carcinogenesis)ņŚÉņä£ ņ┤łĻĖ░ņŚÉ ņØ╝ņ¢┤ļéśļŖö Ļ▓āņØĖņ¦Ć, ņĢäļŗłļ®┤ ņ£äņĀÉļ¦ē ņāüĒö╝ņäĖĒżņØś ņĢöņä▒ ļ│ĆĒÖś ĒøäņŚÉ Ļ░ÉņŚ╝ņØ┤ ņØ╝ņ¢┤ļéśļŖö Ļ▓āņØĖņ¦ĆņŚÉ ļīĆĒĢ┤ņä£ļÅä ļģ╝ļ×ĆņØĆ ņ׳ņ¦Ćļ¦ī, EBVaGCņØś Ļ▒░ņØś ļ¬©ļōĀ ņóģņ¢æņäĖĒżĻ░Ć EBVņŚÉ ĻĘĀņØ╝ĒĢśĻ▓ī Ļ░ÉņŚ╝ļÉśņ¢┤ ņ׳ņ£╝ļ®┤ņä£ ļŗ©Ēü┤ļĪĀņä▒(monoclonality)ņØś EBV DNAļź╝ ļéśĒāĆļé┤ļŖö Ļ▓āņ£╝ļĪ£ ļ│┤ņĢä ņāüĒö╝ņäĖĒżĻ░Ć ņĢģņä▒ņ£╝ļĪ£ ļ│ĆĒśĢļÉśĻĖ░ ņØ┤ņĀäņŚÉ ļ░öņØ┤ļ¤¼ņŖż Ļ░ÉņŚ╝ņØ┤ ņäĀĒ¢ēĒĢĀ Ļ▓āņ£╝ļĪ£ ņČöņĀĢĒĢ£ļŗż[7].
EBV ņ×Āļ│Ą Ļ░ÉņŚ╝(latent infection)ņØĆ ņ×Āļ│Ą ņ£ĀņĀäņ×É(latent gene)ņØś Ēæ£ĒśäĒśĢņŚÉ ļö░ļØ╝ 3Ļ░Ćņ¦Ć ņĢäĒśĢņ£╝ļĪ£ ļéśļłäņ¢┤ņ¦ĆļŖöļŹ░, EBVaGCņŚÉņä£ļŖö EBV encoded small RNAs (EBERs), Epstein-Barr nuclear antigen-1 (EBNA-1), BamHI-A rightward transcripts (BARTs), BART miRNAĻ░Ć ļéśĒāĆļéśļ®░, ņĢĮ ļ░ś ņłśņŚÉņä£ latent membrane protein-2A (LMP-2A)Ļ░Ć ļ░£ĒśäļÉśņ¢┤ ņ×Āļ│Ą ņĀ£1ĒśĢ ļśÉļŖö ņĀ£2ĒśĢ(latency type 1 or 2)ņØä ļéśĒāĆļéĖļŗż(Table 2) [8]. EBNA-1ņØĆ ņäĖĒżņé¼ļ®ĖĻ│╝ ņłÖņŻ╝ļ®┤ņŚŁļ░śņØæņØä ņĀĆĒĢ┤ĒĢśĻ│Ā genome ļČłņĢłņĀĢĒÖöļź╝ ņ£ĀļÅäĒĢśņŚ¼ ņäĖĒżņØś ņ┤łĻĖ░ ļ│ĆĒśĢņŚÉ ņŻ╝ņÜöĒĢ£ ņŚŁĒĢĀņØä ĒĢśļŖö ļ░śļ®┤, LMP-2AļŖö phosphatase and tensin homolog (PTEN)Ļ│╝ Ļ░ÖņØĆ ņóģņ¢æņ¢ĄņĀ£ņ£ĀņĀäņ×É(tumor suppressor gene)ļź╝ ņ¢ĄņĀ£ĒĢśņŚ¼ ņäĖĒż ņ”ØņŗØĻ│╝ ņØ┤ļÅÖņŚÉ Ļ┤ĆņŚ¼ĒĢ©ņ£╝ļĪ£ņŹ© ņ╣©ņŖĄņä▒ ņāüĒö╝ņĢöņŚÉņä£ ņóģņ¢æņØś ņ¦äĒ¢ēņØä ņ┤ēņ¦äĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[9].
2. ļČäņ×ÉņĀü ĒŖ╣ņä▒
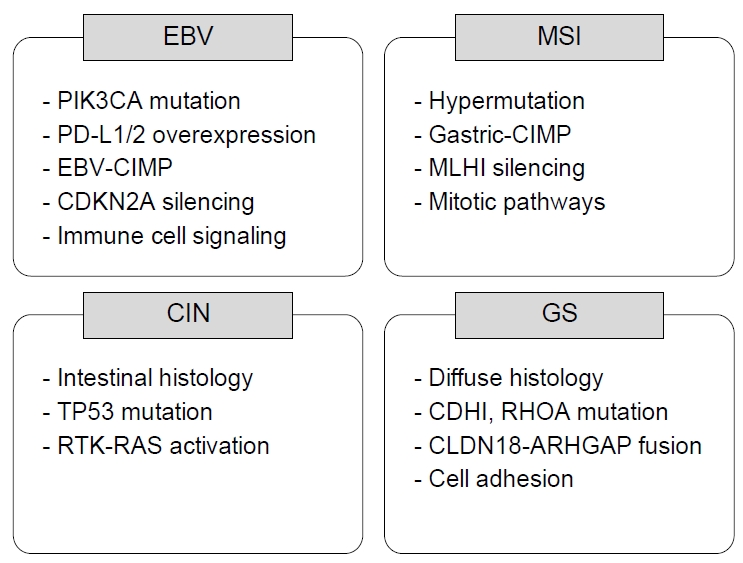
EBVaGCļŖö ņ×äņāüļ│æļ”¼ĒĢÖņĀüņ£╝ļĪ£ ĒŖ╣ņØ┤ĒĢ£ ņä▒Ē¢źņØä ļ│┤ņØ┤ļŖöļŹ░, ņØ┤Ļ▓āņØĆ ļŗżļźĖ ņ£ĀĒśĢņØś ņ£äņäĀņĢöĻ│╝ļŖö ņĢö ļ░£ņāØ ĻĖ░ņĀäņØ┤ ļŗżļź┤ĻĖ░ ļĢīļ¼Ėņ£╝ļĪ£ ņāØĻ░üĒĢ£ļŗż. 2014ļģä ļ░£Ēæ£ļÉ£ Cancer Genome Atlas (TCGA) projectļŖö ņóģĒĢ®ņĀüņØĖ ļČäņ×ÉņĀü ļČäņäØ(comprehensive molecular analysis)ņØä ĒåĄĒĢ┤ ņ£äņäĀņĢöņØä ļŗżņØīņØś 4Ļ░Ćņ¦Ć ņĢäĒśĢņ£╝ļĪ£ ļČäļźśĒĢśņśĆļŗż(Fig. 1) [10]: 1) EBVaGC, 2) gastric carcinoma with microsatellite instability (MSI), 3) gastric carcinoma with chromosomal instability, 4) genetically stable gastric carcinoma. EBVaGCļŖö ļŗżļźĖ ņĢäĒśĢĻ│╝ļŖö ļŗżļź┤Ļ▓ī ļåÆņØĆ ļ╣łļÅäņØś DNA hypermethylationņØä ļ│┤ņØ┤ļ®┤ņä£ CpG island methylator phenotype ļ░£ĒśäņØ┤ ļåÆņĢśņ£╝ļ®░, ĒŖ╣Ē׳ CDKN2A (p16INK4A) promoter hypermethylationņØä Ļ▒░ņØś ļ¬©ļōĀ Ļ▓ĮņÜ░ņŚÉņä£ ĒÖĢņØĖĒĢĀ ņłś ņ׳ņŚłļŗż[10]. ļśÉĒĢ£ EBVaGCņØś 80%ņŚÉņä£ PIK3CA mutationņØ┤ Ļ┤Ćņ░░ļÉśņŚłņ£╝ļ®░, JAK2, CD274 (programmed death-ligand [PD-L] 1), PDCD1LG2 (PD-L2)ņØś ņ”ØĒÅŁĻ│╝ ARID1A (55%)ņÖĆ BCOR (23%) ņ£ĀņĀäņ×É ļ│ĆņØ┤ļÅä ĒØöĒĢśĻ▓ī ļ│┤ņØ┤ļŖö Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│ĀĒĢśņśĆļŗż[10]. ļ░śļ®┤ TP53 Ļ│╝ļ░£ĒśäņØ┤ļéś MSIņÖĆņØś Ļ┤ĆļĀ©ņä▒ņØĆ ļ¦żņÜ░ ļé«ņØĆ Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[6]. ņØ┤ļ¤¼ĒĢ£ ļČäņ×ÉņĀü ĒŖ╣ņä▒ņØś ņ░©ņØ┤Ļ░Ć ļŗżļźĖ ņĢäĒśĢĻ│╝ļŖö ļŗżļźĖ ĻĖ░ņĀäņ£╝ļĪ£ ņĢö ļ░£ņāØĻ│╝ ņ¦äĒ¢ēņŚÉ Ļ┤ĆņŚ¼ĒĢśņŚ¼ ĒŖ╣ņ¦ĢņĀüņØĖ ņ×äņāüļ│æļ”¼ĒĢÖņĀü ņåīĻ▓¼ņØä ļéśĒāĆļé╝ Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż.
3. ņ£äĒŚśņØĖņ×É
ņĄ£ĻĘ╝ 39Ļ░£ņØś ĒÖśņ×É-ļīĆņĪ░ĻĄ░ ņŚ░ĻĄ¼(case-control study)ļź╝ ļČäņäØĒĢ£ ļ®öĒāĆļČäņäØņŚÉ ļö░ļź┤ļ®┤ EBVaGCņØś ņ£äĒŚśļÅäļŖö ņ¦ĆņŚŁņŚÉ ļö░ļØ╝ ļŗżļź┤ļ®░, ņ£äņĢö ļ░£ņāØļźĀņØ┤ ļåÆņØĆ ĻĘ╣ļÅÖ ņĢäņŗ£ņĢä ņ¦ĆņŚŁņŚÉņä£ ļåÆņĢśļŗż[11]. ĒØĪņŚ░ļÅä EBVaGCņØś ļ░£ņāØņØś ņ£äĒŚśņØĖņ×ÉļĪ£ ņĢīļĀżņĀĖ ņ׳ņ£╝ļ®░, ļ╣äĒØĪņŚ░ņ×ÉņÖĆ ļ╣äĻĄÉĒĢśņśĆņØä ļĢī Ēśäņ×¼ ĒØĪņŚ░ņ×É(current smoker)ņŚÉņä£ 2.4ļ░░, Ļ│╝Ļ▒░ ĒØĪņŚ░ņ×É(former smoker)ņŚÉņä£ 2ļ░░ ņĀĢļÅä EBVaGCņØś ļ░£ļ│æņØ┤ ļåÆļŗż[12]. ļśÉĒĢ£, human immunodeficiency virusļéś Helicobacter pylori (H. pylori)ņÖĆ ļÅÖļ░ś Ļ░ÉņŚ╝ļÉ£ Ļ▓ĮņÜ░ņŚÉņä£ ņ£äņĢö ļ░£ņāØņØ┤ ņ”ØĻ░ĆĒĢĀ ņłś ņ׳ļŖöļŹ░[4], ĒĢ£ ņŚ░ĻĄ¼ņŚÉ ļö░ļź┤ļ®┤ H. pyloriņÖĆ EBVņØś ņżæļ│Ą Ļ░ÉņŚ╝ņØ┤ ņØ╝ņ¢┤ļé£ Ļ▓ĮņÜ░ņŚÉ Ļ░üĻ░üņØś ļŗ©ļÅģ Ļ░ÉņŚ╝ņŚÉ ļ╣äĒĢśņŚ¼ ņżæņ”Ø ņ£äņŚ╝(severe polymorphonuclear and mononuclear cell infiltration according to Sydney system)Ļ│╝ņØś ņŚ░Ļ┤Ćņä▒ņØ┤ ņ£ĀņØśĒĢśĻ▓ī ļåÆņĢśļŗż[13]. ņØ┤ļŖö H. pyloriņÖĆ EBVņØś ņżæļ│Ą Ļ░ÉņŚ╝ņŚÉņä£ ņĪ░ņ¦ü ņåÉņāüņØä ņØ╝ņ£╝ĒéżļŖö Ļ░üĻ░üņØś ņŚ╝ņ”Øļ░śņØæņØ┤ ļŗ©ņł£Ē׳ ļŹöĒĢ┤ņ¦ä Ļ▓░Ļ│╝ņØĖņ¦Ć H. pyloriņÖĆ EBV ņ£ĀņĀäņ×É ņé¼ņØ┤ņØś ļ░ĆņĀæĒĢ£ ņāüĒśĖņ×æņÜ®ņ£╝ļĪ£ ņØĖĒĢ£ Ļ▓āņØĖņ¦ĆņŚÉ ļīĆĒĢ┤ņä£ļŖö ļ¬ģĒÖĢĒĢśņ¦Ć ņĢŖņ£╝ļ®░, ņØ╝ļČĆ ņŚ░ĻĄ¼[14]ļŖö EBVņÖĆ H. pylori Ļ░äņØś ņāüĒśĖ ņŚ░Ļ┤ĆņØ┤ ņŚåņŚłļŗżĻ│Ā ĒĢśņŚ¼ ņØ┤ņŚÉ ļīĆĒĢ┤ņä£ļŖö ņóĆ ļŹö ņŚ░ĻĄ¼Ļ░Ć ĒĢäņÜöĒĢĀ Ļ▓āņ£╝ļĪ£ ļ│┤ņØĖļŗż. ņØ┤ņĀä ĒĢ£ ņŚ░ĻĄ¼ļŖö ņ£äĻČżņ¢æ ļ│æļĀźņØ┤ EBVaGCņØś ņ£äĒŚśņØä ņ”ØĻ░Ćņŗ£Ēé©ļŗżĻ│Ā ĒĢśņśĆņ£╝ļ®░, ņ£ä ņĀłņĀ£ņłĀ Ēøä ņ×öņ£äņŚÉņä£ ļ░£ņāØĒĢ£ ņ£äņĢö Ļ░ĆņÜ┤ļŹ░ 35%Ļ░Ć EBVaGCņśĆņØīņØä ĻĘ╝Ļ▒░ļĪ£ ĒĢśņŚ¼ EBVaGCņØś ļ░£ņāØņŚÉ ņ׳ņ¢┤ ņ£äņĀÉļ¦ēņØś ĒÖöĒĢÖņĀü ņåÉņāüņØ┤ ņżæņÜöĒĢ£ ņÜöņØĖņ×äņØä ņĀ£ņŗ£ĒĢśņśĆļŗż[15]. ļśÉ ļŗżļźĖ ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņĢģņä▒ ļ╣łĒśł(pernicious anemia)ņØ┤ ņ׳ļŖö ĒÖśņ×ÉņŚÉņä£ EBVaGCņØś ļ╣łļÅäĻ░Ć 2ļ░░ ņĀĢļÅä ļåÆņĢä ņ£äņČĢņä▒ ņ£äņŚ╝Ļ│╝ ņĢģņä▒ ļ╣łĒśłņØ┤ ļ░£ņāØņØä ņ”ØĻ░Ćņŗ£ĒéżļŖö ņÜöņØĖņØ╝ Ļ▓āņ£╝ļĪ£ ņŻ╝ņןĒĢśņśĆļŗż[16].
4. ņ×äņāüļ│æļ”¼ĒĢÖņĀü ĒŖ╣ņ¦Ģ
EBVaGCļŖö ņĀäņ▓┤ ņ£äņĢö Ļ░ĆņÜ┤ļŹ░ ņĢĮ 10% (1.3~20.1%)ļĪ£ ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ņ£╝ļ®░, ļé©ņä▒ņŚÉņä£ 2~3ļ░░ ņĀĢļÅä ļ░£ņāØ ļ╣łļÅäĻ░Ć ļåÆĻ│Ā, ĒŖ╣Ē׳ ņĀŖņØĆ ņŚ░ļĀ╣ņŚÉņä£ ĒØöĒĢśĻ▓ī ļ░£Ļ▓¼ļÉ£ļŗż[4]. ĒŖ╣ņĀĢ ņ¦ĆņŚŁņŚÉņä£ ĒśĖļ░£ĒĢśļŖö ļ▓äĒéżĒŖĖ ļ”╝ĒöäņóģņØ┤ļéś ļ╣äņØĖļæÉņĢöĻ│╝ļŖö ļŗ¼ļ”¼ ņĀä ņäĖĻ│äņĀü ļČäĒżļź╝ ļ│┤ņØ┤ļéś ņĀäņ▓┤ ņ£äņĢöņŚÉņä£ EBVaGCĻ░Ć ņ░©ņ¦ĆĒĢśļŖö ļ╣äņ£©ņØĆ ņ¦ĆņŚŁļ│äļĪ£ ņ░©ņØ┤ļź╝ ļ│┤ņØ┤ļŖöļŹ░, ņÜ░ļ”¼ļéśļØ╝ņØś Ļ▓ĮņÜ░ ņĀäņ▓┤ ņ£äņĢöņØś 5.6~13%ņŚÉņä£ EBV Ļ░ÉņŚ╝Ļ│╝ ņŚ░Ļ┤Ćņä▒ņØ┤ ņ׳ņØīņØä ļ│┤Ļ│ĀĒĢśņśĆļŗż[5].
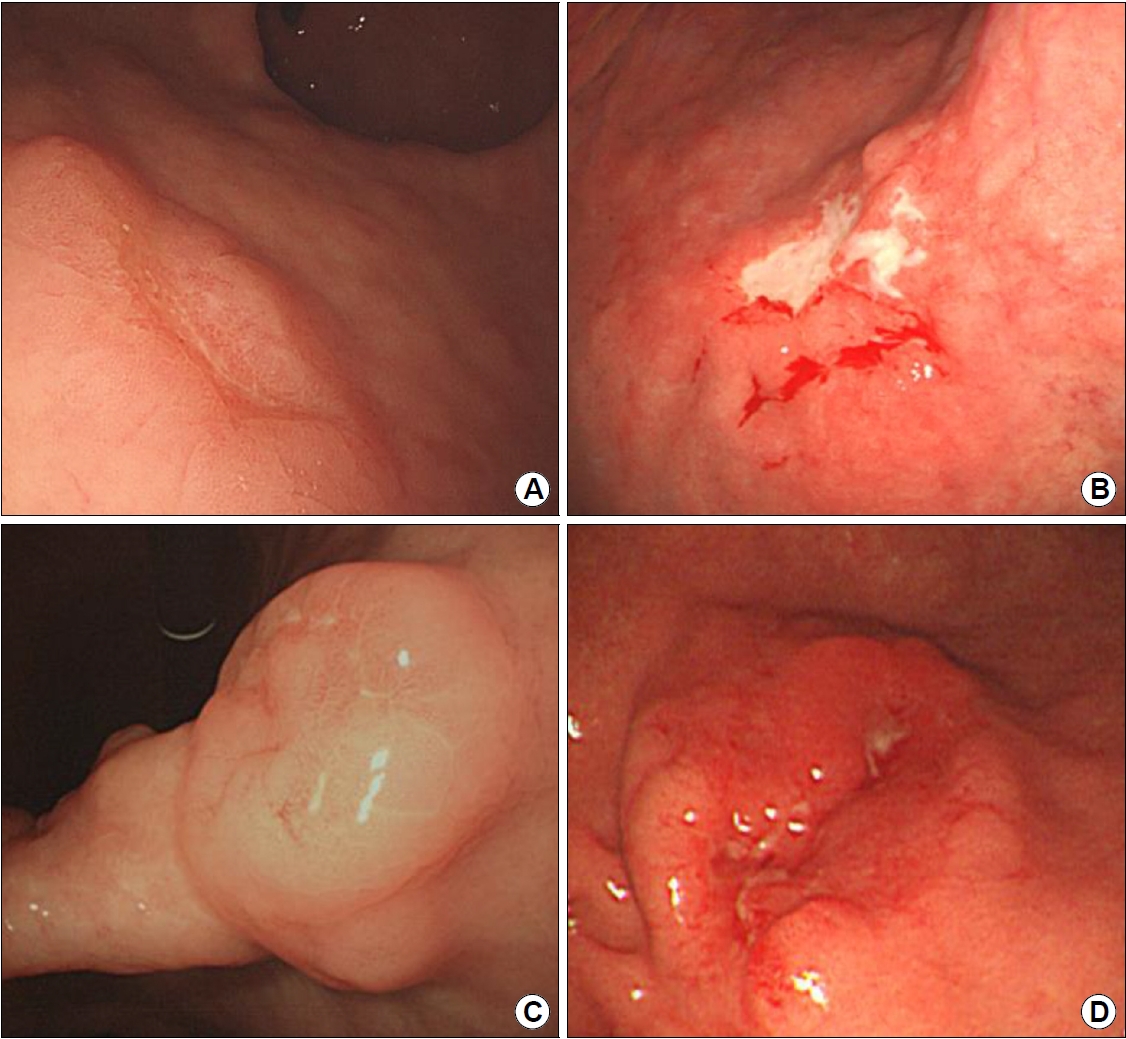
ņ£ä ĻĘ╝ņ£äļČĆņŚÉņä£ ļ¦ÄņØ┤ ļ░£ņāØĒĢśĻ│Ā, ĻĄŁļé┤ņØś ĒĢ£ ļ│┤Ļ│ĀņŚÉ ļö░ļź┤ļ®┤ EBVaGCņØś 84.4%Ļ░Ć ņ£äņØś ņżæņāüļČĆņŚÉ ņ£äņ╣śĒĢśņśĆļŗż[17]. Lauren ļČäļźśļ▓ĢņŚÉ ļö░ļźĖ ņĪ░ņ¦üĒĢÖņĀü ĒśĢĒā£ļŖö ļ»Ėļ¦īĒśĢ(diffuse type)ņØ┤ ĒØöĒĢśļ®░, World Health Organization ļČäļźśļ▓ĢņŚÉ ļö░ļź┤ļ®┤ ņżæļō▒ļÅä-ņĀĆļČäĒÖö(moderate to poorly differentiated) ņäĀņĢöņØś ĒŖ╣ņä▒ņØä ļ│┤ņØ┤ļŖöļŹ░ ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ļŖö EBVaGCņØś 76.2%Ļ░Ć ņĀĆļČäĒÖö ņ£äņĢöņ×äņØä ļ│┤Ļ│ĀĒĢśņśĆļŗż[4]. ĒŖ╣ņ¦ĢņĀüņ£╝ļĪ£ ļ”╝ĒöäņāüĒö╝ņóģņä▒ ņĢöņóģ(lymphoepithelioma-like carcinoma, LELC)ņØ┤ļØ╝Ļ│ĀļÅä ļČłļ”¼ļŖö ļ”╝Ēöäņä▒ ĻĖ░ņ¦łņØä Ļ░Ćņ¦ä ņ£äņĢöņóģ(gastric carcinoma with lymphoid stroma, GCLS)ņØś 80%ņŚÉņä£ EBV ņ¢æņä▒ņØä ļ│┤ņØ┤ļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[18]. GCLSļŖö ņĀäņ▓┤ ņ£äņĢöņŚÉņä£ļŖö 1~4%ļź╝ ņ░©ņ¦ĆĒĢśļŖö ļō£ļ¼Ė ņĪ░ņ¦üĒśĢņ£╝ļĪ£ ļ”╝ĒöäĻĄ¼ ņ╣©ņ£ż(lymphoid infiltration)ņØ┤ ļÅÖļ░śļÉ£ ĒŖ╣ļ│äĒĢ£ ĒśĢĒā£ņØś ņ£äņĢöņóģņØ┤ļŗż. ļ╣äĻ▓░ĒĢ®ņĪ░ņ¦üņä▒ Ļ░äņ¦łņŚÉ ļ¦ÄņØĆ ļ”╝ĒöäĻĄ¼ ļ░Å ĒśĢņ¦łņäĖĒżĻ░Ć ļ»Ėļ¦īņä▒ņ£╝ļĪ£ ņĀä ņóģņ¢æņŚÉ Ļ▒Ėņ│É ņØ╝ņĀĢĒĢśĻ▓ī ņ╣©ņ£żļÉśņ¢┤ ņ׳Ļ│Ā, ļŗżņ¢æĒĢ£ ļ░░ņŚ┤ņØä ļ│┤ņØ┤ļŖö ļ╣äĻĄÉņĀü ņ×æņØĆ ņ¢æņØś ņóģņ¢æņäĖĒżĻ░Ć ņé¼ņØ┤ņé¼ņØ┤ņØś Ļ░äņ¦łņŚÉ ņØśĒĢ┤ ļéśļłĀņ¦ĆļŖö ļ¬©ņ¢æ(lace-like or small nested patten)ņØä Ļ░Ćņ¦äļŗż[19]. ņØ┤ļ¤¼ĒĢ£ ļ”╝Ēöäņä▒ ĻĖ░ņ¦łļ░śņØæņØĆ ņŻ╝ļĪ£ ņäĖĒż ļÅģņä▒ CD8+ Tļ”╝ĒöäĻĄ¼ņŚÉ ņØśĒĢ┤ ņØ╝ņ¢┤ļéśļŖöļŹ░, EBV ņ×Éņ▓┤ņŚÉ ļīĆĒĢ£ ņ¦üņĀæļ░śņØæņØ┤ĻĖ░ļ│┤ļŗżļŖö EBVņŚÉ Ļ░ÉņŚ╝ļÉ£ ņäĖĒżņŚÉ Ēæ£ĒśäļÉ£ ļ░öņØ┤ļ¤¼ņŖż ĒĢŁņøÉņŚÉ ļīĆĒĢ£ ĒĢŁņøÉ-ĒĢŁņ▓┤ļ░śņØæ, ņ”ē ņłÖņŻ╝ ņäĖĒżļ®┤ņŚŁļ░śņØæ(host cellular immune response)ņØ┤ ĒÖ£ņä▒ĒÖöļÉ£ Ļ▓░Ļ│╝ļĪ£ ņśłņāüĒĢ£ļŗż[20]. ļ”╝ĒöäĻĄ¼ ņ╣©ņ£ż ņĀĢļÅäņŚÉ ļö░ļØ╝ EBVaGCļź╝ typical LELC, CrohnŌĆÖs disease-like lymphocytic reaction (CLR), conventional type adenocarcinoma (CA)ņØś ņäĖ Ļ░Ćņ¦Ć ņ£ĀĒśĢņ£╝ļĪ£ ļČäļźśĒĢĀ ņłś ņ׳ņ£╝ļ®░, ņØ╝ļ░śņĀüņ£╝ļĪ£ GCLSļŖö typical LELCņŚÉ CLR ņĪ░ņ¦üĒśĢņØä ĒżĒĢ©ĒĢ£ Ļ░£ļģÉņ£╝ļĪ£ ļ░øņĢäļōżņŚ¼ņ¦ĆĻ│Ā ņ׳ļŗż(Fig. 2) [20].
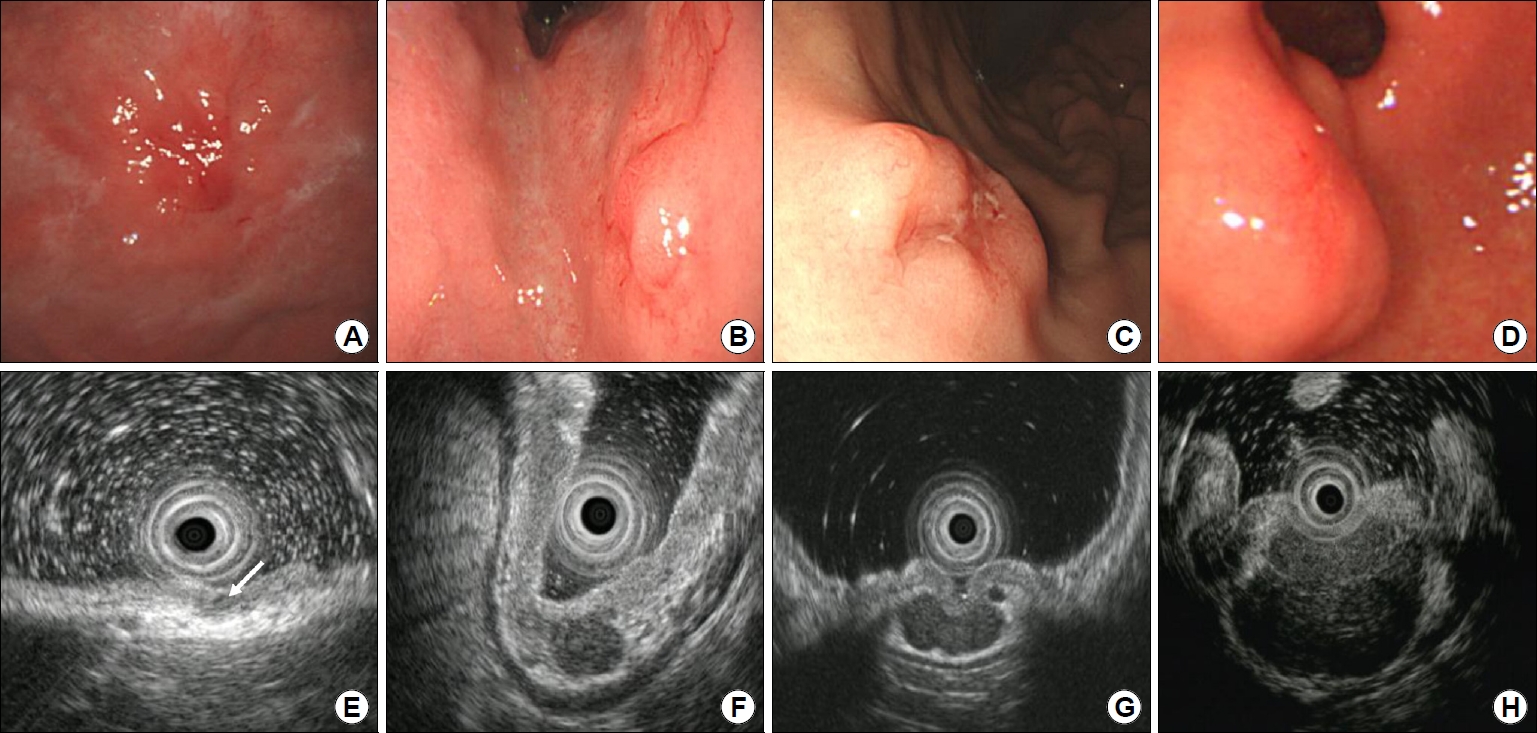
EBVaGCļŖö ņ£ĪņĢłņĀüņ£╝ļĪ£ Ēæ£ļ®┤ ĒĢ©ļ¬░ĒśĢ(superficially depressed) ļśÉļŖö ĻČżņ¢æĒśĢ(ulcerative)ņØ┤ ĒØöĒĢśļ®░, ļ¦ÄņØĆ Ļ▓ĮņÜ░ņŚÉņä£ ņ£äļ▓Į ļ╣äĒøäĻ░Ć ļæÉļō£ļ¤¼ņ¦Ćļ®┤ņä£ ņĀÉļ¦ēĒĢśņóģņ¢æ ņ£Āņé¼ ņ£äņĢö(submucosal tumor-like carcinoma)ņØś ĒśĢĒā£ļĪ£ ļ│┤ņØĖļŗż(Fig. 3) [21]. ņØ┤ļ¤¼ĒĢ£ ņ£ĪņĢłĒśĢņØĆ ņóģņ¢æņäĖĒżņŚÉ ļÅÖļ░śļÉ£ ĒÆŹļČĆĒĢ£ ļ”╝Ēöäņä▒ ĻĖ░ņ¦łļĪ£ ņØĖĒĢśņŚ¼ ļ░£ņāØĒĢśļ®░ ļé┤ņŗ£Ļ▓Į ņ┤łņØīĒīīņŚÉņä£ ĒŖ╣ņ¦ĢņĀüņØĖ ņĀĆņŚÉņĮöņä▒ ņĀÉļ¦ēĒĢś Ļ▓░ņĀł(hypoechoic submucosal nodule)ņØä Ļ┤Ćņ░░ĒĢĀ ņłś ņ׳ļŗż(Fig. 4) [22,23].
5. ņ¦äļŗ©
EBVaGCļź╝ ņ¦äļŗ©ĒĢśĻĖ░ ņ£äĒĢ┤ņä£ļŖö ņóģņ¢æņäĖĒżņŚÉņä£ EBVĻ░Ć Ļ▓ĆņČ£ļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż. ņĪ░ņ¦üņŚÉņä£ņØś EBV Ļ▓ĆņČ£ņØĆ ņĀ£ņ×Éļ”¼ļČĆĒĢ®ļ▓Ģ(in situ hybridization, ISH)Ļ│╝ ņżæĒĢ®ĒÜ©ņåīņŚ░ņćäļ░śņØæ(polymerase chain reaction, PCR)ņØä ņØ┤ņÜ®ĒĢśņŚ¼ ļŗżņØīņØś ņ¦äļŗ© Ēæ£ņ¦Ćņ×É(diagnostic marker)ļź╝ ĒÖĢņØĖĒĢ£ļŗż: 1) small RNA EBER1/EBER2 for ISH, 2) EBNA-1, Bam-M, BamHI-W viral antigens for PCR [24]. ņØ╝ļ░śņĀüņØĖ ņ£ĀņĀäļ¼╝ņ¦ł Ļ▓ĆņČ£ņŚÉļŖö ņ£ĀņĀäņ×É ņ”ØĒÅŁņØ┤ ņłśļ░śļÉśļŖö PCRņØ┤ ļ»╝Ļ░ÉļÅäĻ░Ć ļåÆņ¦Ćļ¦ī, ņóģņ¢æ ņĪ░ņ¦üļé┤ ņ×Āļ│Ą Ļ░ÉņŚ╝ļÉ£ Bļ”╝ĒöäĻĄ¼ņŚÉ ņØśĒĢ┤ ņ£äņ¢æņä▒ņØä ņ┤łļלĒĢśĻĖ░ļÅä ĒĢ£ļŗż. ņØ┤ļ¤¼ĒĢ£ ņØ┤ņ£ĀļĪ£ ISH ļ░®ļ▓ĢņØ┤ ļ╣äĻĄÉņĀü ļ»╝Ļ░ÉļÅäļŖö ļé«ņ¦Ćļ¦ī EBVaGCļź╝ ņ¦äļŗ©ĒĢśļŖö ļŹ░ ņ׳ņ¢┤ Ēæ£ņżĆ ņ¦äļŗ©ļ▓Ģ(gold standard)ņØ┤ļØ╝ ĒĢśĻ▓Āļŗż[24].
6. ņśłĒøä
EBV ņØīņä▒ ņ£äņĢöĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ ņóģņ¢æņØś ņ╣©ņ£ż ņĀĢļÅä(T stage)ņÖĆ ļ”╝ĒöäņĀł ņĀäņØ┤(N state) ļ╣łļÅäĻ░Ć ļé«ņĢä ņØ╝ļ░śņĀüņ£╝ļĪ£ ņóŗņØĆ ņśłĒøäļź╝ ļ│┤ņØĖļŗż[4]. ņĪ░ĻĖ░(early stage) EBVaGCņŚÉņä£ņØś ļ”╝ĒöäņĀł ņĀäņØ┤ņ£©ņØĆ ņĀÉļ¦ēņĢöĻ│╝ ņĀÉļ¦ēĒĢś ņ╣©ņ£żņĢöņŚÉņä£ Ļ░üĻ░ü 2.2~4.2%ņÖĆ 14.0~23.6%ļĪ£ ļ│┤Ļ│ĀļÉśņŚłĻ│Ā[17], ĒĢ£ ļ®öĒāĆļČäņäØņŚÉ ļö░ļź┤ļ®┤ EBVaGC ĒÖśņ×ÉĻĄ░ņŚÉņä£ ņāØņĪ┤ ĻĖ░Ļ░äņØś ņżæņĢÖĻ░Æ(median survival time)ņØ┤ ĻĖĖņŚłļŗż(8.5ļģä vs. 5.3ļģä) [25]. ļŗżļźĖ ņŚ░ĻĄ¼ņŚÉņä£ļÅä EBVaGC ĒÖśņ×ÉĻĄ░ņŚÉņä£ ļīĆņĪ░ĻĄ░ļ│┤ļŗż 1ĻĖ░ ĒÖśņ×ÉņØś ļ╣äņ£©ņØ┤ ļŹö ļ¦Äņ£╝ļ®┤ņä£(37.4% vs. 4.9%), ļŹö ļéśņØĆ ņāØņĪ┤ņ£©ņØä ļ│┤ņ×äņØä ņŻ╝ņןĒĢśņśĆļŗż(5-year overall survival rate: 71.4% vs. 56.1%; 5-year disease-free survival rate: 67.5% vs. 55.2%) [20]. TCGA projectņŚÉ ļö░ļØ╝ ņ£äņĢöņØä ļČäļźśĒĢśņŚ¼ ļČäņäØĒĢ£ ņĄ£ĻĘ╝ ĻĄŁļé┤ ņŚ░ĻĄ¼ņŚÉņä£ļÅä ņ¦äĒ¢ēņä▒ EBVaGC ĒÖśņ×ÉņŚÉņä£ ĒÖöĒĢÖņÜöļ▓Ģ(chemotherapy) Ēøä ņĀäņ▓┤ ņāØņĪ┤ ĻĖ░Ļ░ä(overall survival)Ļ│╝ ļ¼┤ņ×¼ļ░£ ņāØņĪ┤ ĻĖ░Ļ░ä(relapse-free survival)ņØ┤ ļŹö ļéśņØĆ Ļ▓░Ļ│╝ļź╝ ļ│┤ņŚ¼ņŻ╝ņŚłļŗż[26].
EBVaGCņØś ņśłĒøäļŖö ņóģņ¢æņØś Ēü¼ĻĖ░, ļ”╝ĒöäņĀł ņĀäņØ┤ ņŚ¼ļČĆ ņÖĖņŚÉļÅä ĒÖśņ×ÉņØś ņŚ╝ņ”Øļ░śņØæņØ┤ ņżæņÜöĒĢ£ ņŚŁĒĢĀņØä ĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż. EBVaGCļź╝ ļ”╝ĒöäĻĄ¼ ņ╣©ņ£ż ņĀĢļÅäņŚÉ ļö░ļØ╝ ņĀäĒśĢņĀüņØĖ LELCņÖĆ CLR, CAļĪ£ ļČäļźśĒĢśņśĆņØä ļĢī LELCņÖĆ CLR ņĪ░ņ¦üĒśĢņŚÉņä£ ļŹö ĻĖ┤ ņĀäņ▓┤ ņāØņĪ┤ ĻĖ░Ļ░ä(hazard ratio Ļ░üĻ░ü 0.09ņÖĆ 0.42)Ļ│╝ ļ¼┤ņ¦łļ│æ ņāØņĪ┤ ĻĖ░Ļ░ä(disease-free survival; hazard ratio Ļ░üĻ░ü 0.05ņÖĆ 0.46)ņØä ļ│┤ņśĆļŗż[20]. ņØ┤Ļ▓āņØĆ EBVaGCņØś ņśłĒøäĻ░Ć ĒÖśņ×ÉņØś ņŚ╝ņ”Øļ░śņØæ(host inflammatory response)ņŚÉ ņØśņĪ┤ĒĢ£ļŗżļŖö ĻĘ╝Ļ▒░ļĪ£ņä£ ļ”╝ĒöäĻĄ¼ņä▒ ņ╣©ņ£żņØ┤ ņłÖņŻ╝ņØś ņäĖĒżļ®┤ņŚŁĻ│╝ ņ▓┤ņĢĪņä▒ ļ®┤ņŚŁļ░śņØæņØä ļ░śņśüĒĢśļ®░ ņĢöņäĖĒżņŚÉ ļīĆĒĢ£ ņØ╝ņóģņØś ļ░®ņ¢┤ĻĖ░ņĀäņ£╝ļĪ£ ņ×æņÜ®ĒĢĀ Ļ▓āņ£╝ļĪ£ ņāØĻ░üĒĢ£ļŗż[27]. ņĄ£ĻĘ╝ ņŚ░ĻĄ¼ņŚÉņä£ļÅä EBVaGCņŚÉņä£ ņóģņ¢æņ╣©ņ£żņä▒ ļ”╝ĒöäĻĄ¼(tumor infiltrating lymphocytes, TILs)Ļ░Ć ĒÖśņ×ÉņØś ļ¼┤ņ×¼ļ░£ ņāØņĪ┤ ĻĖ░Ļ░ä(hazard ratio, 12.193)Ļ│╝ ļ¼┤ņ¦łļ│æ ņāØņĪ┤ ĻĖ░Ļ░ä(hazard ratio, 4.836)ņØä Ē¢źņāüņŗ£ņ╝░ņ£╝ļ®░, ļé«ņØĆ TILsņØĆ ĻĄŁņåīļ”╝ĒöäņĀł ņĀäņØ┤ņÖĆ ļéśņü£ ņśłĒøäļź╝ ņśłņĖĪĒĢĀ ņłś ņ׳ļŖö ņØĖņ×ÉļØ╝Ļ│Ā ļ│┤Ļ│ĀĒĢśņśĆļŗż[28]. GCLSņØś ĒśĢĒā£ļź╝ ļ│┤ņØ┤ļŖö EBVaGCĻ░Ć ĒĢŁņĢöņĀ£ņŚÉļÅä ļŹö ņל ļ░śņØæĒĢśļŖö Ļ▓āņ£╝ļĪ£ļÅä ļ│┤Ļ│ĀĒĢśņśĆļŖöļŹ░, ņØ┤ļŖö Ļ░äņ¦łņŚÉ ļ”╝ĒöäĻĄ¼ ņ╣©ņ£żņØ┤ ĒÆŹļČĆĒĢśņŚ¼ ņóģņ¢æ ĻĖ░ņ¦łļé┤ Ļ▓░ņ▓┤ ņĪ░ņ¦üĻ│╝ ņä¼ņ£ĀĒÖöĻ░Ć Ļ▒░ņØś ņŚåĻĖ░ ļĢīļ¼ĖņŚÉ ĒĢŁņĢöņĀ£Ļ░Ć ņóģņ¢æņäĖĒżļĪ£ ļŹö ņל ņ╣©Ēł¼ĒĢĀ ņłś ņ׳ļŗżļŖö ņĀÉĻ│╝ ņóģņ¢æņäĖĒżĻ░Ć EBVņŚÉ Ļ░ÉņŚ╝ļÉ©ņ£╝ļĪ£ņŹ© ĒĢŁņĢöņĀ£ņŚÉ ļīĆĒĢ┤ ļåÆņØĆ ņśłļ»╝ļÅäļź╝ Ļ░Ćņ¦ĆĻ▓ī ļÉ£ Ļ▓āņ£╝ļĪ£ ņČöņĖĪĒĢ£ļŗż[29].
7. ņ×äņāüņĀü ņØśņØś
EBVaGCļŖö ļīĆļČĆļČäņŚÉņä£ ļ»Ėļ¦īĒśĢ ļśÉļŖö ņĀĆļČäĒÖö ņäĀņĢöņØś ņĪ░ņ¦üĒśĢņØä ļ│┤ņØ┤ĻĖ░ ļĢīļ¼ĖņŚÉ ņĪ░ĻĖ░ ņ£äņĢöņØ┤ļØ╝ ĒĢśļŹöļØ╝ļÅä Gotoda ļō▒[31]ņØ┤ ņĀ£ņŗ£ĒĢ£ ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ņłĀņØś ņØ╝ļ░śņĀüņØĖ ņĀüņØæņ”ØņØ┤ ļÉśņ¦Ć ņĢŖļŖöļŗż. ĒĢśņ¦Ćļ¦ī GCLSņØś ĒśĢĒā£ļź╝ ļ│┤ņØ┤ļŖö ņĪ░ĻĖ░ ņ£äņĢö(early gastric carcinoma with lymphoid stroma, EGCLS)ņØś Ļ▓ĮņÜ░ņŚÉņä£ļŖö ļČäĒÖöņĢöĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ ļ”╝ĒöäņĀł ņĀäņØ┤ņØś ņ£äĒŚśņØ┤ Ļ░ÖĻ▒░ļéś ņśżĒ׳ļĀż ļŹö ļé«ļŗżĻ│Ā ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ņ£╝ļ®░ ņĀÉļ¦ēĒĢś ņ╣©ņ£żņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ņŚÉņä£ļÅä ļ”╝ĒöäņĀł ņĀäņØ┤ņØś ļ╣łļÅäĻ░Ć ļ¦żņÜ░ ļé«ņĢśļŗż[23,32,33]. ĻĄŁļé┤ ņŚ░ĻĄ¼ļōżņŚÉņä£ļÅä EGCLSņØś ņ╣©ņ£ż Ļ╣ŖņØ┤ņŚÉ ļö░ļźĖ ļ”╝ĒöäņĀł ņĀäņØ┤ ņŚ¼ļČĆļź╝ ļČäņäØĒĢśņśĆņØä ļĢī SM1/SM2 ņ╣©ņ£żņĢöņŚÉņä£ ļ”╝ĒöäņĀł ņĀäņØ┤Ļ░Ć ļ░£Ļ▓¼ļÉśņ¦Ć ņĢŖņĢśļŗż[23,32]. ņØ┤ļ¤¼ĒĢ£ Ļ▓░Ļ│╝ļź╝ ņóģĒĢ®ĒĢ┤ ļ│┤ļ®┤ EGCLSņØś ņĪ░ņ¦üĒśĢņØä ļ│┤ņØ┤ļŖö EBVaGCņØś Ļ▓ĮņÜ░ņŚÉņä£ ļ»Ėļ¦īĒśĢņØś ņĪ░ņ¦üĒśĢņØä ļ│┤ņØ┤Ļ▒░ļéś ņĀÉļ¦ēĒĢś ņ╣©ņ£żņØ┤ ņ׳ļŗż ĒĢśļŹöļØ╝ļÅä ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ņłĀņØ┤ ĒÜ©Ļ│╝ņĀüņØĖ ņ╣śļŻīĻ░Ć ļÉĀ ņłś ņ׳ņØīņØä ņĪ░ņŗ¼ņŖżļ¤ĮĻ▓ī ņāØĻ░üĒĢ┤ļ│╝ ņłś ņ׳ļŗż. ĒĢśņ¦Ćļ¦ī ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ņłĀņØś ņĀüņØæņ”Øņ£╝ļĪ£ ņĀĢļ”ĮļÉśĻĖ░ ņ£äĒĢ┤ņä£ļŖö ņóĆ ļŹö ļ¦ÄņØĆ ņĀäĒ¢źņĀü ņŚ░ĻĄ¼Ļ░Ć ĒĢäņÜöĒĢśļ®░, Ēśäņ×¼ļĪ£ņä£ļŖö ĻĖ░ņĀĆņ¦łĒÖśņ£╝ļĪ£ ņØĖĒĢśņŚ¼ ņĀäņŗĀ ņāüĒā£Ļ░Ć ņóŗņ¦Ć ņĢŖņØĆ ĒÖśņ×É ļśÉļŖö ņ£äņĀäņĀłņĀ£ņłĀņØś ļČĆļŗ┤ņØ┤ ņ׳ļŖö ĒÖśņ×ÉņŚÉņä£ ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ņłĀņØä ĒÜ©Ļ│╝ņĀüņØĖ ļīĆņĢłņ£╝ļĪ£ Ļ│ĀļĀżĒĢ┤ļ│╝ ņłś ņ׳Ļ▓Āļŗż.
ĒĢ£ĒÄĖ EBVaGCļŖö ļ®┤ņŚŁņøÉņä▒(immunogenicity)ņØ┤ ļåÆņØĆ ņ£äņĢöņ£╝ļĪ£ PD-L1/PD-L2ņØś ļ░£ĒśäņØ┤ ļåÆĻ│Ā, CD8+ TILsĻ░Ć ĒÆŹļČĆĒĢśņŚ¼ ļ®┤ņŚŁĻ┤Ćļ¼Ėņ¢ĄņĀ£ņĀ£(immune check point inhibitor)ņŚÉ ļ░śņØæņØ┤ ņóŗņØä Ļ▓āņ£╝ļĪ£ ĻĖ░ļīĆļÉśņ¢┤ ņÖöļŗż[27]. Anti-PD-L1 antibodyņØĖ pembrolizumabņØä ņé¼ņÜ®ĒĢ£ phase II trialņØĆ PD-L1 ņ¢æņä▒ ņ£äņĢö ĒÖśņ×ÉņŚÉņä£ PD-L1 ņØīņä▒ ņ£äņĢö ĒÖśņ×ÉņÖĆ ļ╣äĻĄÉĒĢśņŚ¼ ņĢĮņĀ£ņØś ņĀäņ▓┤ ļ░śņØæļźĀ(overall response rate)ņØ┤ ļåÆņĢśņØī(15.5% vs. 5.5%)ņØä ļ│┤Ļ│ĀĒĢśņśĆĻ│Ā, nivolumabņØä ņØ┤ņÜ®ĒĢ£ phase III trialņŚÉņä£ļŖö EBVaGC ĒÖśņ×ÉņØś ņĀäņ▓┤ ņāØņĪ┤ ĻĖ░Ļ░äņØś ņżæņĢÖĻ░Æ(median overall survival)ņØ┤ Ē¢źņāüļÉ£ Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż(5.3 vs. 4.1 months) [4]. ņØ┤ ņÖĖņŚÉļÅä PIK3K ņ¢ĄņĀ£ņĀ£ļéś demethylating agentņØś ņ╣śļŻī ĒÜ©Ļ│╝ļź╝ ĒÖĢņØĖĒĢśĻĖ░ ņ£äĒĢ£ ņŚ░ĻĄ¼ļōżļÅä ņŗ£ļÅäļÉśĻ│Ā ņ׳ņ¦Ćļ¦ī, Ēśäņ×¼Ļ╣īņ¦Ć ņØ╝Ļ┤ĆļÉ£ Ļ▓░Ļ│╝ļź╝ ļ│┤ņŚ¼ņŻ╝Ļ│Ā ņ׳ņ¦Ć ņĢŖņĢä ĒøäņåŹ ņŚ░ĻĄ¼ļōżņØś Ļ▓░Ļ│╝ļź╝ ĻĖ░ļŗżļĀż ļ│┤ņĢäņĢ╝ ĒĢĀ Ļ▓āņØ┤ļŗż.
Ļ▓░ ļĪĀ
EBVaGCļŖö ļŗżļźĖ ņ£ĀĒśĢņØś ņ£äņĢöĻ│╝ļŖö ļŗżļźĖ ņ£ĀņĀäņĀü, ņ×äņāüļ│æļ”¼ĒĢÖņĀü ĒŖ╣ņä▒ņØä ļ│┤ņØ┤ļ®░, ĒŖ╣ņ¦ĢņĀüņ£╝ļĪ£ GCLS ĒśĢĒā£ņØś ņĪ░ņ¦üĒśĢņØä Ļ┤Ćņ░░ĒĢĀ ņłś ņ׳ļŗż. GCLSņŚÉņä£ ļÅÖļ░śļÉśļŖö ļ”╝ĒöäĻĄ¼ņä▒ ĻĖ░ņ¦łņØĆ EBV Ļ░ÉņŚ╝ ņóģņ¢æņäĖĒżņŚÉ ļīĆĒĢ£ ņØ╝ņóģņØś ņłÖņŻ╝ļ®┤ņŚŁļ░śņØæņ£╝ļĪ£ ĒĢŁņóģņ¢æ ĒÜ©Ļ│╝(anti-tumor effect)ļź╝ ļéśĒāĆļé┤ņ¢┤ EBVaGCņØś ņóŗņØĆ ņśłĒøäņÖĆ ņŚ░Ļ┤ĆļÉ£ ņØĖņ×ÉļĪ£ ņāØĻ░üĒĢ£ļŗż. GCLSņØś 80%ņŚÉņä£ EBV ņ¢æņä▒ņØä ļ│┤ņØ┤ĻĖ░ ļĢīļ¼ĖņŚÉ GCLSņØś ņĪ░ņ¦üĒśĢņØä ļ│┤ņØ┤ļŖö ņ£äņĢö ņĪ░ņ¦üņŚÉņä£ EBVļź╝ ņ¦äļŗ©ĒĢśļŖö Ļ▓āņØ┤ ĒĢäņÜöĒĢ£ļŹ░, EBER ISHĻ░Ć EBVaGCļź╝ ņ¦äļŗ©ĒĢśļŖö ņĀüĒĢ®ĒĢ£ Ēæ£ņżĆ Ļ▓Ćņé¼ļ▓ĢņØ┤ļŗż. ņ×äņāüņĀüņØĖ ņĖĪļ®┤ņŚÉņä£ GCLSņØś ņĪ░ņ¦üĒśĢņØä ļ│┤ņØ┤ļŖö ņĪ░ĻĖ░ EBVaGCņØś Ļ▓ĮņÜ░ ļŗżļźĖ ņ£ĀĒśĢņØś ņĢöĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ ļ”╝ĒöäņĀł ņĀäņØ┤ņ£©ņØ┤ ļ¦żņÜ░ ļé«ĻĖ░ ļĢīļ¼ĖņŚÉ ņĀÉļ¦ēĒĢś ņ╣©ņ£żņØ┤ ņ׳ļŗż ĒĢśļŹöļØ╝ļÅä ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ņłĀņØś ĒÜ©Ļ│╝ņĀüņØĖ ļīĆņāüņ£╝ļĪ£ Ļ│ĀļĀżĒĢ┤ ļ│╝ ņłś ņ׳ņ£╝ļ®░, ņ¦äĒ¢ēņä▒ EBVaGCņØś Ļ▓ĮņÜ░ PD-L1ņØś ļ░£ĒśäņØ┤ ļåÆņĢä ļ®┤ņŚŁĻ┤Ćļ¼Ėņ¢ĄņĀ£ņĀ£ ņ╣śļŻī ĒÜ©Ļ│╝ņŚÉ ļīĆĒĢ£ ĻĖ░ļīĆļź╝ ĒĢśĻ│Ā ņ׳ņ£╝ļ®░ ļ¦ÄņØĆ ļ®┤ņŚŁņ¢ĄņĀ£ņĀ£ ņ╣śļŻī ņŚ░ĻĄ¼ļź╝ ņ¦äĒ¢ēĒĢśĻ│Ā ņ׳ļŗż. Ļ▓░ļĪĀņ£╝ļĪ£ EBVļŖö ņ£äņĢö ņ¦äļŗ©ņŚÉ ņ׳ņ¢┤ ņśłĒøäļź╝ ņśłņĖĪĒĢśĻ│Ā ņ╣śļŻī Ļ│äĒÜŹņØä Ļ▓░ņĀĢĒĢśļŖö ņāłļĪ£ņÜ┤ ņāØņ▓┤Ēæ£ņ¦Ćņ×É(novel biomarker)ļĪ£ņä£ ņżæņÜöĒĢśĻ│Ā, EBVaGCņŚÉņä£ ņŗżņĀ£ ņśłĒøäļź╝ Ē¢źņāüņŗ£Ēé¼ ņłś ņ׳ļŖö ņāłļĪ£ņÜ┤ Ēæ£ņĀü ĒĢŁņøÉņØś Ļ░£ļ░£Ļ│╝ ņŚ░ĻĄ¼Ļ░Ć ĒĢäņÜöĒĢśļŗż.