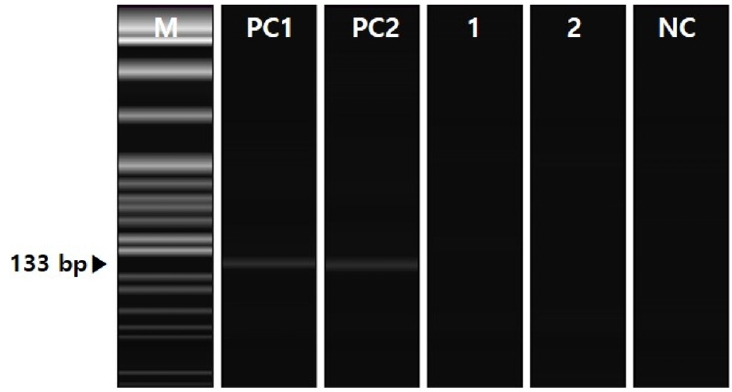
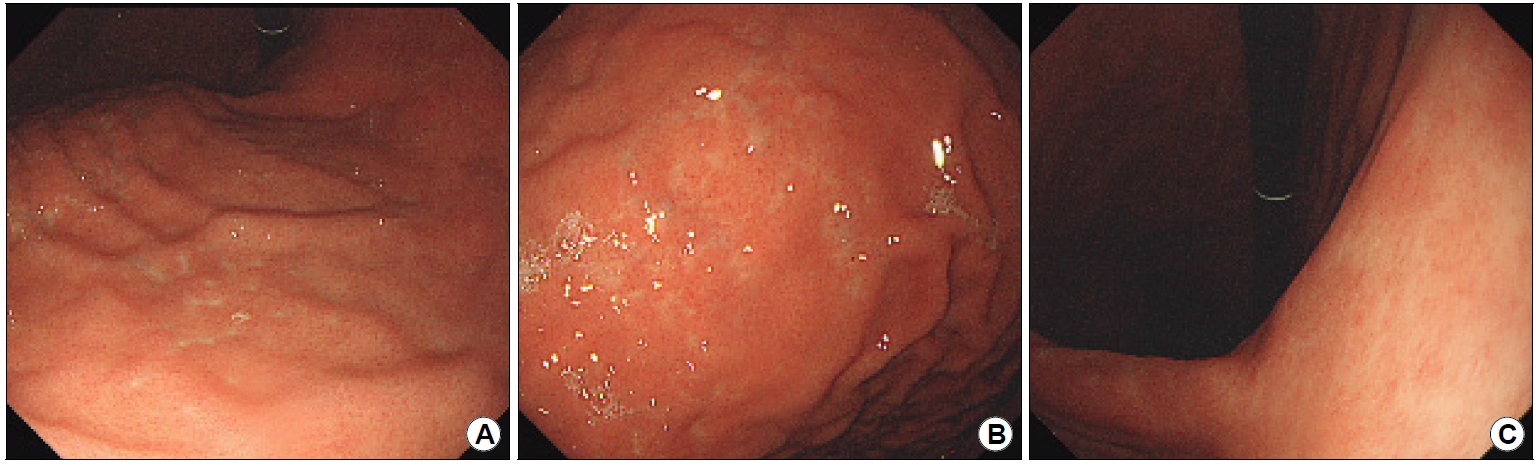
ņÜöņĢĮ: 29ņäĖ ļé©ņ×ÉĻ░Ć 4Ļ░£ņøöĻ░ä 7 kgņØś ņ▓┤ņżæ Ļ░ÉņåīĻ░Ć ņ׳ņ¢┤ ņŗ£Ē¢ēĒĢ£ ņ£äļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ņŚÉņä£ ņØ┤ņāü ņåīĻ▓¼ņØä ļ│┤ņŚ¼ ļ│æņøÉņŚÉ ņÖöļŗż. ņ▓┤ņżæ Ļ░Éņåī ņØ┤ņÖĖņŚÉ ļŗżļźĖ ņ”ØņāüņØĆ ņŚåņŚłņ£╝ļ®░ ņĢĮļ¼╝ ļ│ĄņÜ®ļĀźņØ┤ļéś ļ│æļĀźļÅä ņŚåņŚłļŗż. ņĪ░ļČĆĻ░Ć ļīĆņןņĢöņ£╝ļĪ£ ņ¦äļŗ©ļ░øņØĆ Ļ░ĆņĪ▒ļĀźņØ┤ ņ׳ņŚłļŗż. ņ£äļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢ£ Ļ▓░Ļ│╝, ļČäļ¼ĖļČĆņÖĆ ņāüļČĆ ņ▓┤ļČĆņŚÉņä£ ļ¼┤ņłśĒ׳ ļ¦ÄņØĆ ņ×æņØĆ ĒØ░ņāē ĒĢ©ļ¬░ĒśĢ ļ»Ėļ×ĆļōżņØ┤ ļ│┤ņśĆļŗż(Fig. 1A). ņ£äņŻ╝ļ”äņŚÉņä£ļŖö ļŗżļ░£ņä▒ Ēśłņä▒ ļ░śņĀÉņ£╝ļĪ£ ĻĄ¼ņä▒ļÉ£ ņĀÉņāü ļ░£ņĀü(spotty redness)ņØ┤ Ļ┤Ćņ░░ļÉśņŚłļŗż(Fig. 1B). ņ£äĻ░üņØś Ēøäļ▓ĮņŚÉņä£ļŖö ļ»ĖņäĖĒśłĻ┤Ć ņ”ØņŗØĻ│╝ ņØ┤ņĀä ņĪ░ņ¦ü Ļ▓Ćņé¼ļĪ£ ņØĖĒĢ£ ĒØ░ņāē ĒØēĒä░Ļ░Ć Ļ┤Ćņ░░ļÉśņŚłļŗż(Fig. 1C). ņĀäņĀĢļČĆņŚÉņä£ļŖö ĻĘĀņØ╝ĒĢ£ ĒśłĻ┤Ćņāü(regular arrangement of collecting venules)ņØ┤ Ļ┤Ćņ░░ļÉśņŚłļŗż(Fig. 1D). ņ£äņ▓┤ļČĆņØś ļīĆļ¦īņĖĪĻ│╝ ņ£äĻ░üņØś Ēøäļ▓ĮņĖĪņŚÉņä£ ņĪ░ņ¦ü Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśņśĆļŗż(Fig. 2). Giemsa ņŚ╝ņāēņŚÉņä£ Helicobacter pylori (H. pylori)ļŖö Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśņ£╝ļ®░ ņÜöņåīĒśĖĻĖ░ Ļ▓Ćņé¼ļÅä ņØīņä▒ņØ┤ņŚłļŗż. Ēśłņ▓Ł Ļ▓Ćņé¼ņŚÉņä£ ĒĢŁH. pylori immunoglobulin G (IgG) ņłśņ╣śļŖö <5 AU/mLļĪ£ ņØīņä▒, ĒÄ®ņŗ£ļģĖĻ▓É(pepsinogen, PG) I ņłśņ╣śļŖö 36.0 ng/mL, PG II ņłśņ╣śļŖö 9.5 ng/mL, PG I/II ļ╣äļŖö 3.8ļĪ£ ņĀĢņāü ņåīĻ▓¼ņØä ļ│┤ņśĆļŗż. H. pyloriĻ░Ć ņĢäļŗī Helicobacter (non-H. pylori Helicobacter, NHPH) Ļ░ÉņŚ╝ņØä ņ¦äļŗ©ĒĢśĻĖ░ ņ£äĒĢ┤ ĻĘĀņŚ╝ĻĖ░ņä£ņŚ┤ ļČäņäØ(pyrosequencing analysis)ņØä ņŗ£Ē¢ēĒĢśņśĆļŗż(Fig. 3). ņ£äļé┤ņŗ£Ļ▓ĮņŚÉņä£ Ļ┤Ćņ░░ļÉ£ Ļ┤æļ▓öņ£äĒĢ£ ļ│æļ│ĆņØś ņ¦äļŗ©ņØĆ ļ¼┤ņŚćņØĖĻ░Ć?
ĒĢ┤ņäż: H. pylori ņØīņä▒ņ£╝ļĪ£ ņ¦äļŗ©ĒĢśĻĖ░ ņ£äĒĢ┤ņä£ļŖö ņ╣©ņŖĄņĀüņØĖ Ļ▓Ćņé¼ņÖĆ ļ╣äņ╣©ņŖĄņĀüņØĖ Ļ▓Ćņé¼ņŚÉņä£ ļ¬©ļæÉ ņØīņä▒ ņåīĻ▓¼ņØä ļ│┤ņŚ¼ņĢ╝ ĒĢśļ®░, ņĀĢņāü ĒśłĻ┤ĆņāüņØ┤ ļ│┤ņØ╝ Ļ▓ĮņÜ░ņŚÉļŖö H. pylori ļ»ĖĻ░ÉņŚ╝ņ×ÉņØ╝ Ļ░ĆļŖźņä▒ņØ┤ 32.2ļ░░ ņāüņŖ╣ĒĢ£ļŗż[1]. ļ░śļīĆļĪ£ ņāüļČĆ ņ▓┤ļČĆņŚÉņä£ Ļ┤æļ▓öņ£äĒĢ£ ļ░£ņĀüņØ┤ ļ│┤ņØ╝ Ļ▓ĮņÜ░ņŚÉļŖö H. pylori Ļ░ÉņŚ╝ņ×ÉņØ╝ Ļ░ĆļŖźņä▒ņØ┤ 26.8ļ░░ ņāüņŖ╣ĒĢśļ®░, ņØ┤ļŖö ĒÖ£ļÅÖņä▒ H. pylori Ļ░ÉņŚ╝ņØä ņŗ£ņé¼ĒĢśļŖö ĒŖ╣ņ¦ĢņĀüņØĖ ņåīĻ▓¼ņ£╝ļĪ£ NHPH Ļ░ÉņŚ╝ņä▒ ņ£äņŚ╝ņŚÉņä£ ļ│┤Ļ│ĀļÉ£ ņĀüņØ┤ ņŚåļŗż[2]. Helicobacter suis ļō▒ņØś NHPH Ļ░ÉņŚ╝ņØĆ ņĪ░ĻĖ░ņ£äņĢö(early gastric cancer, EGC) ĒśĢĒā£ņØś ņĢģņä▒ ņóģņ¢æ, Ļ▓░ņĀłņä▒ ņ£äņŚ╝, ņåīĒÖöņä▒ ĻČżņ¢æ, ņ£äĻ░üņØä ņżæņŗ¼ņ£╝ļĪ£ ĒĢ£ ļīĆļ”¼ņäØ ļ¬©ņ¢æņØś Ļ▓Įļ»ĖĒĢ£ ņ£äņČĢņä▒ ņ£äņŚ╝, ņĀäņĀĢļČĆņØś ļČłĻĘĀņØ╝ĒĢ£ ļ░£ņĀüņØ┤ļéś ļ»Ėļ×Ć ļō▒ņØĆ ņ£Āļ░£ĒĢĀ ņłś ņ׳ņ¦Ćļ¦ī H. pylori Ļ░ÉņŚ╝ņ▓śļ¤╝ Ļ┤æļ▓öņ£äĒĢ£ ļ░£ņĀüņØ┤ļéś ņŻ╝ļ”ä ļ╣äļīĆļŖö ņ£Āļ░£ĒĢśņ¦Ć ļ¬╗ĒĢ£ļŗż[3].
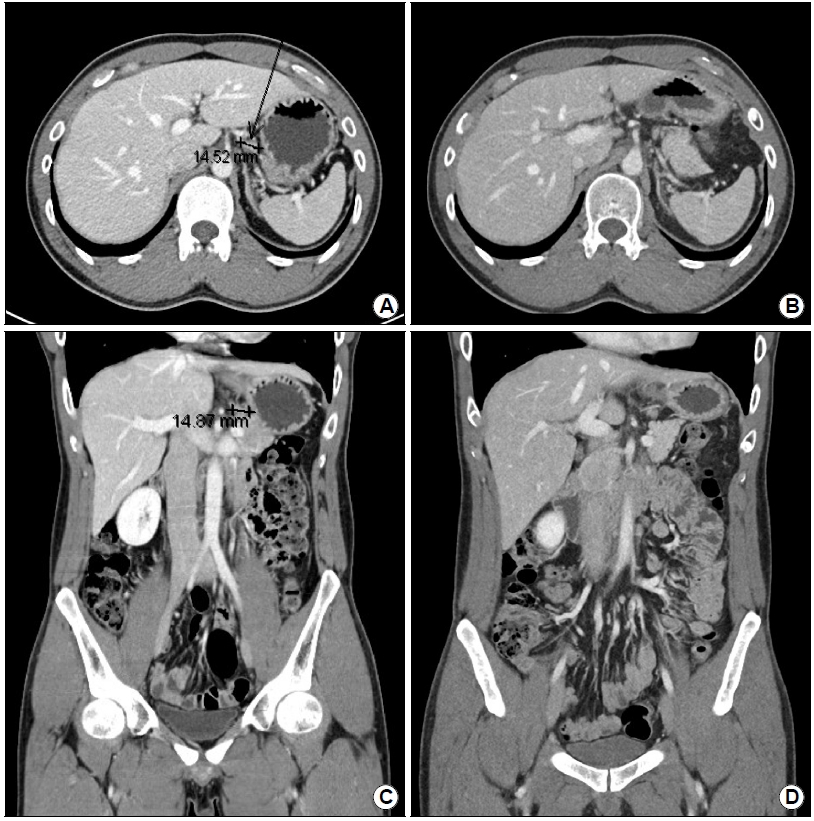
ņØ┤ ņ”ØļĪĆļŖö ņāüļČĆ ņ▓┤ļČĆņØś ļīĆļ¦īņĖĪņØä ņżæņŗ¼ņ£╝ļĪ£ H. pylori ĒÖ£ļÅÖņä▒ Ļ░ÉņŚ╝ņØä ņŗ£ņé¼ĒĢśļŖö ņĀÉņāü ļ░£ņĀüņØ┤ Ļ┤Ćņ░░ļÉśņŚłņ£╝ļéś ļ╣äņ╣©ņŖĄņĀüņØĖ Ļ▓Ćņé¼ņÖĆ ņ╣©ņŖĄņĀüņØĖ Ļ▓Ćņé¼ ļ¬©ļæÉņŚÉņä£ H. pylori ņØīņä▒ņ£╝ļĪ£ ļ│┤Ļ│ĀļÉśņŚłņ£╝ļ®░ NHPHļÅä ņ¦äļŗ©ļÉśņ¦Ć ņĢŖņØĆ ļō£ļ¼Ė Ļ▓ĮņÜ░ņØ┤ļŗż. ļ®┤ņŚŁņŚ╝ņāē Ļ▓░Ļ│╝ņŚÉņä£ CD20 ņ¢æņä▒, CK ļ”╝ĒöäņāüĒö╝ļ│æļ│Ć ņ¢æņä▒, Ki-67 3~5% ņ¢æņä▒, Bcl-2 ņ¢æņä▒, Bcl-6 ņØīņä▒, CD10 ņØīņä▒, CD3 ņØīņä▒ņ£╝ļĪ£ ļ│┤Ļ│ĀļÉśņ¢┤ H. pylori ņØīņä▒ņØĖ ņ£ä ļ¦ÉĒŖĖ ļ”╝Ēöäņóģ(mucosa-associated lymphoid tissue [MALT] lymphoma)ņ£╝ļĪ£ ņ¦äļŗ©ĒĢśņśĆļŗż. ĒśłņĢĪ Ļ▓Ćņé¼ņŚÉņä£ ņĀ¢ņé░ĒāłņłśĒÜ©ņåī(lactate dehydrogenase) ņłśņ╣śļŖö 336 IU/L (ņ░ĖĻ│Āņ╣ś 263~450 IU/L)ņśĆņ£╝ļ®░ ĒØēļČĆņÖĆ ļ│ĄļČĆ ņ╗┤Ēō©Ēä░ļŗ©ņĖĄņ┤¼ņśü(CT)ņŚÉņä£ ņ£äņØś ņóīņĖĪ ļ”╝ĒöäņĀłņØ┤ 1.5 cmļĪ£ ņĖĪņĀĢļÉśņŚłļŗż(Fig. 4A, B). ļ│æĻĖ░ļŖö Ann Arbor stage II1E, ĻĄŁņĀ£ņśłĒøäņ¦ĆĒæ£(international prognostic index, IPI)ļŖö ļé«ņØĆ IPI ņ£äĒŚśļÅäļĪ£ ĒīÉļŗ©ļÉśņŚłļŗż. Clonal IgH gene rearrangementļŖö ņŚåņŚłņ£╝ļ®░ apoptosis inhibitor 2 (API2)-MALT lymphoma-associated translation 1 (MALT1) chimera ņ£ĀņĀäņ×ÉņÖĆ ņŚ░Ļ┤ĆļÉ£ ņŚ╝ņāēņ▓┤ ņĀäņ£ä 11q21: t(11;18) (q21;q21)ļÅä ļ░£Ļ▓¼ļÉśņ¦Ć ņĢŖņĢśļŗż.
10% ļ»Ėļ¦īņØś ņ£ä ļ¦ÉĒŖĖ ļ”╝ĒöäņóģņØĆ NHPH Ļ░ÉņŚ╝ņØ┤ļéś ņŚ╝ņāēņ▓┤ ņĀäņ£ä ļśÉļŖö ņ×ÉĻ░Ćļ®┤ņŚŁņ¦łĒÖśņŚÉ ņØśĒĢ┤ ļ░£ņāØĒĢśļŖö H. pylori ņØīņä▒ ļ”╝Ēöäņóģņ£╝ļĪ£ ņ¦äļŗ©ļÉ£ļŗż[4]. Ļ░Ćņן ĒØöĒĢ£ ņøÉņØĖņØĆ NHPH Ļ░ÉņŚ╝ņ£╝ļĪ£ ņØ╝ļČĆļŖö H. pylori ņĀ£ĻĘĀ ņ╣śļŻīņŚÉ ļ░śņØæĒĢśņ¦Ćļ¦ī[5], API2-MALT1 ņ¢æņä▒ņØ┤ļ®┤ Ļ┤ĆĒĢ┤ņ£©ņØ┤ ļé«ļŗż[6]. ĻĄŁļé┤ņŚÉņä£ Ļ░Ćņן ļ¦ÄņØĆ ņ£ä ļ¦ÉĒŖĖ ļ”╝Ēöäņóģ ĒÖśņ×É 345ļ¬ģņØä ļČäņäØĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ļŖö 57.1%ņØś H. pylori ņØīņä▒ ņ£ä ļ¦ÉĒŖĖ ļ”╝ĒöäņóģņØ┤ ņĀ£ĻĘĀ ņ╣śļŻīļĪ£ Ļ┤ĆĒĢ┤ļÉśņŚłļŗż[7]. ļ®öĒāĆļČäņäØ ņŚ░ĻĄ¼ņŚÉ ņØśĒĢśļ®┤ ņĀ£ĻĘĀ ņ╣śļŻī ĒøäņØś H. pylori ņØīņä▒ ņ£ä ļ¦ÉĒŖĖ ļ”╝ĒöäņóģņØś Ļ┤ĆĒĢ┤ņ£©ņØĆ 29.3% (95% CI, 22.2~37.4%)ļĪ£[8], ĒĢ£ĻĄŁņŚÉņä£ Ļ┤ĆĒĢ┤ņ£©ņØ┤ Ļ░Ćņן ļåÆĻ│Ā ņØ╝ļ│ĖņŚÉņä£ Ļ░Ćņן ļé«ļŗż[9]. ņØ╝ļ│ĖņØ┤ ļé«ņØĆ ņØ┤ņ£ĀļŖö ņ╣©ņŖĄņĀüņØĖ Ļ▓Ćņé¼, Ēśłņ▓Ł ĒĢŁH. pylori IgG, ņÜöņåīĒśĖĻĖ░ Ļ▓Ćņé¼ļ┐Éļ¦ī ņĢäļŗłļØ╝ ļīĆļ│ĆĒĢŁņøÉ Ļ▓Ćņé¼ņÖĆ Ēśłņ▓Ł PG Ļ▓Ćņé¼Ļ╣īņ¦Ć ļ¬©ļæÉ ņØīņä▒ ņåīĻ▓¼ņØä ļ│┤ņŚ¼ņĢ╝ H. pylori ņØīņä▒ņ£╝ļĪ£ ņ¦äļŗ©ĒĢśĻĖ░ ļĢīļ¼Ėņ£╝ļĪ£ ņČöņĀĢļÉ£ļŗż. Ēśłņ▓Ł PG I ņłśņ╣śĻ░Ć 70 ng/mL ņØ┤ĒĢśņØ┤ļ®┤ņä£ PG I/II ļ╣äĻ░Ć 3.0 ņØ┤ĒĢśļĪ£ Ēśłņ▓ŁĒĢÖņĀü ņ£äņČĢņØ┤ ļ│┤Ļ│ĀļÉśļ®┤ H. pylori ņØīņä▒ņØ┤ ņĢäļŗī Ļ│╝Ļ▒░ Ļ░ÉņŚ╝ņ×ÉļĪ£ ļČäļźśĒĢśļ»ĆļĪ£[10], ņÜ░ļ”¼ļéśļØ╝ņŚÉņä£ļŖö H. pylori ņØīņä▒ņØĖ ņóģņ¢æņØ┤ ņØ╝ļ│ĖņŚÉņä£ļŖö Ļ│╝Ļ▒░ Ļ░ÉņŚ╝ņ£╝ļĪ£ ņØĖĒĢ┤ ļ░£ņāØĒĢ£ H. pylori ņŚ░Ļ┤Ćņä▒ ņóģņ¢æņ£╝ļĪ£ ņ¦äļŗ©ļÉśļŖö Ļ▓ĮĒ¢źņØ┤ ņ׳ļŗż.
ņ£ä ļ¦ÉĒŖĖ ļ”╝ĒöäņóģņØś ļ│æĻĖ░ļŖö ņ╣śļŻīņŚÉ ļīĆĒĢ£ ļ░śņØæņØä ņśłņĖĪĒĢśļŖö ļŹ░ ņ׳ņ¢┤ņä£ ņżæņÜöĒĢśļ®░, H. pylori ņ¢æņä▒ņØĖ IEĻĖ░ļéś II1EĻĖ░ņØś ņ£ä ļ¦ÉĒŖĖ ļ”╝ĒöäņóģņØĆ ņĀ£ĻĘĀņÜöļ▓ĢņØ┤ļéś ņĀüņØĆ ņ¢æ(25.2 Gy)ņØś ļ░®ņé¼ņäĀ ņ╣śļŻīļĪ£ Ļ┤ĆĒĢ┤ļÉĀ ņłś ņ׳ļŗż[11]. ņĀ£ĻĘĀ ņ╣śļŻīņŚÉ ļ░śņØæĒĢśļŖö H. pylori ņØīņä▒ ņ£ä ļ¦ÉĒŖĖ ļ”╝ĒöäņóģņØĆ ņŻ╝ļĪ£ ņ£äņØś ņøÉņ£äļČĆņŚÉņä£ ļ░£ņāØĒĢśļ®░ H. pylori Ļ░ÉņŚ╝ņä▒ ņ£ä ļ¦ÉĒŖĖ ļ”╝ĒöäņóģĻ│╝ ņ£Āņé¼ĒĢ£ ĒĢ©ļ¬░ĒśĢ ņĪ░ĻĖ░ņ£äņĢö ņ£Āņé¼ĒśĢ(EGC IIc-like type), ņĀÉļ¦ēĒĢś ņóģņ¢æĒśĢ(submucosal tumor type), ļŗżļ░£ņä▒ ļ»Ėļ×ĆĒśĢ(multiple erosion type), ņĪ░ņĢĮļÅīĒśĢ(cobblestone type), ļČĆļČäņĀüņØĖ ņŻ╝ļ”äļ╣äļīĆĒśĢ(partial giant-fold type), Ēć┤ņāēĒśĢ(discoloration type) ļō▒ņ£╝ļĪ£ Ļ┤Ćņ░░ļÉ£ļŗż[12]. ļ░śļ®┤ņŚÉ ņĀ£ĻĘĀ ņ╣śļŻīņŚÉ ļ░śņØæĒĢśņ¦Ć ņĢŖļŖö H. pylori ņØīņä▒ ņ£ä ļ¦ÉĒŖĖ ļ”╝ĒöäņóģņØĆ ņŻ╝ļĪ£ ņ£äņØś ĻĘ╝ņ£äļČĆņŚÉņä£ ņāüĒö╝ĒĢś ņóģņ¢æņØ┤ļéś ņÜ®ņóģ Ļ░ÖņØĆ ņ£ĄĻĖ░ĒśĢ ļ│æļ│Ćņ£╝ļĪ£ ņ¦äļŗ©ļÉśļ®░ diffuse large B cell lymphomaņÖĆ ņ£Āņé¼ĒĢ£ ļ¬©ņ¢æņ£╝ļĪ£ ņ¦äĒ¢ēĒĢ£ļŗż[13]. ļ░®ņé¼ņäĀ ņ╣śļŻīņŚÉļÅä ļ░śņØæĒĢśņ¦Ć ņĢŖņØä ļĢīļŖö ĒĢŁņĢö ņ╣śļŻīļéś rituximabĻ│╝ Ļ░ÖņØĆ ĒĢŁCD20 ļŗ©Ēü┤ļĪĀĒĢŁņ▓┤ ļ®┤ņŚŁņÜöļ▓ĢņØä Ļ│ĀļĀżĒĢĀ ņłś ņ׳ļŗż[11].
ņØ┤ ņ”ØļĪĆļŖö API2-MALT1 ņØīņä▒Ļ│╝ Helicobacter ņØīņä▒ņØĖ II1E ļ│æĻĖ░ņØś ņ£ä ļ¦ÉĒŖĖ ļ”╝Ēöäņóģņ£╝ļĪ£ ļ░®ņé¼ņäĀ ņ╣śļŻīļź╝ ĻČīĒĢśņśĆņ£╝ļéś ļŹ£ ņ╣©ņŖĄņĀüņØĖ ņĀ£ĻĘĀ ņ╣śļŻīņŚÉ ļīĆĒĢ£ ļ░śņØæņØä ļ©╝ņĀĆ ĒÖĢņØĖĒĢśĻĖĖ ņøÉĒĢśņŚ¼ amoxicillin 1 g, clarithromycin 500 mg, lansoprazole 30 mgņØä ĒĢśļŻ© ļæÉ ļ▓ł ņØ╝ņŻ╝ņØ╝Ļ░ä Ēł¼ņŚ¼ĒĢśņśĆļŗż. ņ£äļé┤ņŗ£Ļ▓Į ņåīĻ▓¼ņØ┤ ņĀ£ĻĘĀ ņ╣śļŻīņŚÉ ļ░śņØæĒĢśļŖö ļŗżļ░£ņä▒ ļ»Ėļ×ĆĒśĢĻ│╝ Ēć┤ņāēĒśĢ ņåīĻ▓¼ņØä ļ│┤ņśĆĻ│Ā, ņĪ░ņ¦ü Ļ▓Ćņé¼ļĪ£ ņŗ£Ē¢ēĒĢ£ NHPH ņ¦äļŗ©ņØ┤ ņ£äņØīņä▒ņØ╝ Ļ░ĆļŖźņä▒ļÅä ņ׳ņ¢┤ņä£ ņĀ£ĻĘĀ ņ╣śļŻīņŚÉ ļ░śņØæĒĢśĻĖĖ ĻĖ░ļīĆĒ¢łņŚłņ£╝ļéś ļæÉ ļŗ¼ ĒøäņØś ņ£äļé┤ņŗ£Ļ▓Į ņĪ░ņ¦ü Ļ▓Ćņé¼ņŚÉņä£ ņ£ä ļ¦ÉĒŖĖ ļ”╝ĒöäņóģņØ┤ ņŚ¼ņĀäĒ׳ ļ│┤Ļ│ĀļÉśņ¢┤ ņ¦Ćņ▓┤ ņŚåņØ┤ ļ░®ņé¼ņäĀ ņ╣śļŻī(30.6 Gy, 17 fractions)ļź╝ ĻČīĒĢśņśĆļŗż. ļ░®ņé¼ņäĀ ņ╣śļŻīļź╝ ļ¦łņ╣£ Ēøä 4Ļ░£ņøö ļÆżņŚÉ ņŗ£Ē¢ēĒĢ£ CT Ļ▓Ćņé¼ņŚÉņä£ ņ×æņĢäņ¦ä ļ”╝ĒöäņĀłņØ┤ ĒÖĢņØĖļÉśņŚłļŗż(Fig. 4C, D). ņ£äļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ņāü ņāüļČĆ ņ▓┤ļČĆņŚÉņä£ Ļ┤Ćņ░░ļÉśļŹś ĒØ░ņāē ĒĢ©ļ¬░ĒśĢ ļ»Ėļ×ĆļōżņØĆ ņØ┤ņĀäņŚÉ ļ╣äĒĢ┤ Ļ░ÉņåīĒĢśņśĆņ£╝ļ®░(Fig. 5A), ņ£äņŻ╝ļ”äņØś ņĀÉņāü ļ░£ņĀüņØĆ ņé¼ļØ╝ņ¦ä ņāüĒā£ņśĆļŗż(Fig. 5B). ņ£äĻ░üņØś Ēøäļ▓ĮņŚÉļŖö ņĪ░ņ¦ü Ļ▓Ćņé¼ĒĢ£ ĒØöņĀüļ¦ī ļé©ņĢäņ׳ņŚłļŗż(Fig. 5C). ņ▓śņØīņŚÉ ļ”╝ĒöäņóģņØ┤ ņ¦äļŗ©ļÉśņŚłļŹś ņ▓┤ļČĆņØś ļīĆļ¦īĻ│╝ ņ£äĻ░üņØś Ēøäļ▓ĮņŚÉņä£ ņČöņĀü ņĪ░ņ¦ü Ļ▓Ćņé¼ļź╝ ĒĢśņśĆņ£╝ļéś ļ¬©ļæÉ ņØīņä▒ņ£╝ļĪ£ ļ│┤Ļ│ĀļÉśņŚłļŗż.
ņóģĒĢ®ĒĢĀ ļĢī, ņØ┤ ņ”ØļĪĆļŖö ļ╣äņ╣©ņŖĄņĀüņØĖ Ļ▓Ćņé¼(Ēśłņ▓Ł Ļ▓Ćņé¼ņÖĆ ņÜöņåīĒśĖĻĖ░ Ļ▓Ćņé¼)ņÖĆ ņ╣©ņŖĄņĀüņØĖ Ļ▓Ćņé¼(H&EņÖĆ Giemsa ņŚ╝ņāē, ĻĘĀņŚ╝ĻĖ░ņä£ņŚ┤ļČäņäØ)ņŚÉņä£ ļ¬©ļæÉ ņØīņä▒ ņåīĻ▓¼ņØä ļ│┤ņØĖ H. pylori ņØīņä▒ ņ£ä ļ¦ÉĒŖĖ ļ”╝Ēöäņóģņ£╝ļĪ£, ĒÖ£ļÅÖņä▒ H. pylori Ļ░ÉņŚ╝ņØä ņŗ£ņé¼ĒĢśļŖö ņĀÉņāü ļ░£ņĀüņØä ļ│┤ņØĖ ĒŖ╣ņØ┤ĒĢ£ ņ”ØļĪĆņØ┤ļŗż. ņ£ĪņĢłņĀüņØĖ ņåīĻ▓¼ņØĆ ņĀ£ĻĘĀ ņ╣śļŻīņŚÉ ņל ļ░śņØæĒĢśļŖö ļŗżļ░£ņä▒ ļ»Ėļ×ĆĒśĢĻ│╝ Ēć┤ņāēĒśĢņØä ļ│┤ņśĆņ£╝ļéś ņĀ£ĻĘĀ ņ╣śļŻīņŚÉ ļ░śņØæĒĢśņ¦Ć ņĢŖņĢäņä£ ļ░®ņé¼ņäĀ ņ╣śļŻīĻ░Ć ĒĢäņÜöĒĢśņśĆļŗż. ņØ┤ņ▓śļ¤╝ ņ£ĪņĢłņĀüņ£╝ļĪ£ļŖö H. pylori Ļ░ÉņŚ╝ņä▒ ņ£ä ļ¦ÉĒŖĖ ļ”╝ĒöäņóģņØä ņØśņŗ¼ĒĢĀ ņłś ņ׳ļŖö ņåīĻ▓¼ņØä ļ│┤ņŚ¼ļÅä ļ░®ņé¼ņäĀ ņ╣śļŻī ĒøäņŚÉņĢ╝ Ļ┤ĆĒĢ┤ļÉ£ H. pylori ņØīņä▒ ņ£ä ļ¦ÉĒŖĖ ļ”╝ĒöäņóģņØä Ļ▓ĮĒŚśĒĢśņśĆĻĖ░ņŚÉ ļ│┤Ļ│ĀĒĢ£ļŗż.