위아전절제술 잔위에 발생한 두꺼운 노란색 삼출성 위막
Thick Yellowish Exudative Pseudomembrane of the Post-subtotal Gastrectomy Residual Stomach
Article information

요약: 80세 남자가 10일 전 시작된 연하통, 연하곤란, 목 이물감으로 거의 먹지 못했다고 입원을 요구하였다. 20일 전부터 식욕부진이 시작되었고, 죽이라도 먹으려면 물을 서너 번 마셔야 삼켜지는 정도였으며, 최근 1주간 약 3 kg의 체중 감소가 동반되었다고 주장하였다. 당뇨병, 고혈압, 폐기종이 있었고 12년 전 진행성 위암으로 빌로스 1형의 위아전절제술을 시행받았다. 키 172.9 cm, 몸무게 53.6 kg이었다. 백혈구 11,400/µL, 혈색소 10.7 g/L, 혈소판 314,000/µL, 혈중요소질소 49.0 mg/dL, 크 레아티닌 1.12 mg/dL였고, 혈청 검사에서 HBs Ag/Ab (-/+), HCV Ab (-), human immunodeficiency virus Ag/Ab (-/-), rapid plasma reagin test (-)였다.
위내시경에서는 위아전절제술 시행한 잔위 전반에 두껍고 불투명한 노란색의 삼출물이 붙어 위막을 형성하고 있었고 주로 대만 측에 더 두껍게 관찰되었으며 십이지장으로 침범하지는 않았다(Fig. 1). 삼출물은 내시경 선단으로 밀었을 때 쉽게 떨어져 나갔고 노출 점막의 부종과 경도의 발적을 동반하였다. 위내시경 진단은 무엇인가?
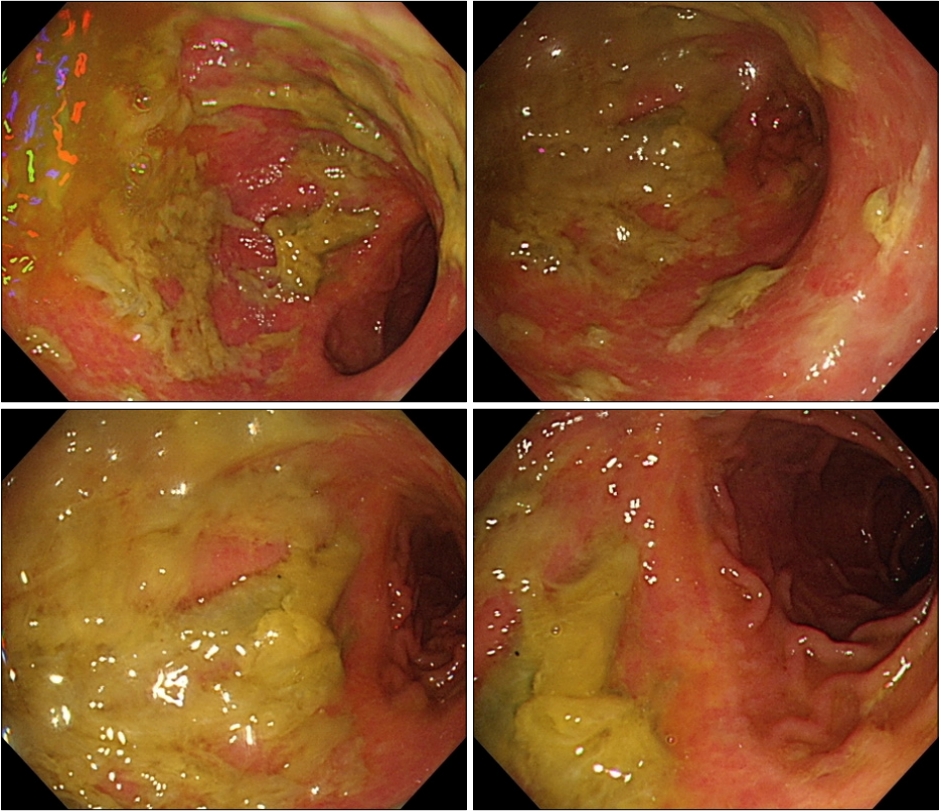
Endoscopic findings of the stomach (subtotal gastrectomy state). Diffuse thick yellowish exudative pseudomembrane adheres to the gastric mucosa. The pseudomembrane falls off easily when pushed with the tip of the endoscope. The exposed mucosa shows edema and mild hyperemia.
해설: 위의 삼출물을 보일 때 삼출성 위염을 먼저 생각하지만 불투명한 노란색의 삼출물이 두꺼운 위막을 형성하며 붙어 있다는 것이 진단의 핵심이 되겠다. 이 환자의 경우는 연하통과 삼킴곤란이 주 증상이었고 심한 전신쇠약이 있어 식도암이나 잔위암 말기를 생각하고 컴퓨터단층촬영을 시행하였으나 뚜렷한 잔위암이나 식도암의 증거는 없었다. 진단의 실마리는 구강과 식도에서 찾을 수 있었다. 볼 점막에 백색 플라크로 생각되는 병변이 있었고, 상부식도 괄약근에 약 0.5 cm 길이로 두꺼운 grade III의 크림 형태의 백색 플라크가 관찰되어 식도 칸디다증에 합당하였고 플라크의 밀도가 상부식도에서 중부로 오면서 grade II에서 grade I으로 감소하는 양상을 보였다(Fig. 2). 식도열공탈장이 있었으며 LA-C 또는 D의 심한 역류성 식도염이 동반되었고 중부 식도에는 얕은 지도상의 궤양을 형성하였다. 이에 위 병변 역시 칸디다증으로 의심하고 잔위 대만부의 두꺼운 위막이 붙은 점막에서 조직 검사를 시행하였다. 중등도의 위축성 위염과 장상피화생이 관찰되었으나 Helicobacter pylori 증거는 찾지 못했고, PAS염색에서 칸디다 속에 합당한 가성균사 소견을 보여 위 칸디다증을 진단할 수 있었다(Fig. 3).

Endoscopic findings of the esophagus. Multiple whitish plaques suggesting candidiasis are seen from the upper esophageal sphincter to mid esophagus. Severe reflux esophagitis is noted with hiatal hernia and shallow geographic ulcer on the mid-esophagus. Histological examination of the geographic ulcer of the mid-esophagus shows only inflamed granulation tissue.

(A-D) Histologic findings of the gastric biopsy specimen. The slide shows moderate chronic gastritis and numerous Candida species hyphae (A: H&E stain, ×100; B: H&E stain, ×200; C: H&E stain, ×400; D: PAS stain, ×400).
식도 칸디다증은 건강검진 내시경의 약 0.32%에서 발견되나[1] 위 칸디다증은 드물어서 아직 체계적인 보고는 없다. 경증인 표재감염형과 중중인 심부침윤형으로 구분할 수 있고, 후자는 위 천공을 유발하는 등 예후가 나쁘며 점막하층과 장막 혈관의 혈전을 유발한다[2]. 위 칸디다증의 내시경 소견은 초기에는 홍반성 점막 변화가 관찰되며 점차 흰색 혹은 황색의 삼출성 위막이 형성되고, 궤양, 용종, 점막 출혈이 관찰될 수 있다[3,4]. 내시경 소견에 따라 백태형, 궤양형, 결절형으로 분류할 수 있고 이 중 백태형이 가장 많다[3,4]. 이 증례에서 두꺼운 삼출성 위막이 노란색을 띄는 것은 위아전절제술 후 역류한 담즙에 의한 착색으로 생각된다.
내시경 직후 니스타틴 시럽과 란소프라졸 붕해정 30 mg을 투여하였는데 투약 직후부터 바로 연하통이 소실되기 시작하였고 다음날 아침 식이 시도에서 식욕부진과 연하곤란이 모두 해결되어 퇴원을 요구할 정도로 호전되었다. 양성자펌프억제제의 작용시간을 생각할 때 투약 초기의 빠른 반응은 니스타틴에 의한 효과가 더 큰 것으로 생각되고, 식욕부진의 호전은 위 병변의 호전과 관련이 있을 것으로 추정된다. 당뇨병과 고혈압 치료제 이외의 약제, 스테로이드 흡입제나 경구 복용은 모두 부인하였기에 이 환자의 기저 질환 중 당뇨병과 위암 수술 상태가 대표적인 위험인자로 생각된다.
현재까지 보고된 위 칸디다증은 보통 위궤양 조직 검사에서 우연히 발견되는 경우가 많고 일반적인 경우는 항진균제 사용없이 궤양 치료로 호전되기에 면역억제 상태가 아니라면 경증의 경과를 보인다[5]. 그러나 심부침윤형으로 발전한 경우 천공을 유발하기도 하므로[2] 고령, 암환자, 항암 치료, 천공 고위험군, 전신 진균감염 가능성이 높은 경우는 진균제를 사용을 고려할 필요가 있다[5].
Notes
No potential conflict of interest relevant to this article was reported.