Clinical Characteristics of Cytomegalovirus Disease of the Upper Gastrointestinal Tract: A 10-Year Multicenter Retrospective Study
Article information

Abstract
Objectives
Gastrointestinal cytomegalovirus (CMV) disease is a major contributor to mortality in immunocompromised patients. Few studies have discussed upper gastrointestinal CMV (UGICMV) disease in immunocompetent patients. We compared the clinical outcomes of UGI-CMV between immunocompromised and immunocompetent patients.
Methods
This retrospective study included patients with UGI-CMV disease from five tertiary hospitals across Korea (2010– 2022). Patients’ clinical data and outcomes were recorded.
Results
UGI-CMV was diagnosed in 54 patients; 27 (50.0%) had esophageal, 24 (44.4%) had gastric, and 3 patients (5.6%) had duodenal involvement. Patients’ median age was 64 years (interquartile range 53–75 years), and the most common comorbidities included hypertension (57.4%) and diabetes (38.9%). The predominant symptom was abdominal pain (46.3%), and the most common endoscopic finding was ulcers (70.4%). Antiviral treatment was administered to 31 patients, and 23 patients underwent observation without treatment. We investigated 32 immunocompromised (59.3%) and 22 immunocompetent (40.7%) patients and observed no intergroup differences in comorbidities and in laboratory and endoscopic findings. Immunocompromised patients had longer length of hospitalization (median 46.2 days vs. 20.0 days, p=0.001). However, treatment outcomes, including the need for intensive care unit admission and mortality did not significantly differ. The overall mortality rate was 13.0%; one patient from the immunocompromised group died of UGI-CMV disease. The treatment success rate was higher in immunocompromised patients who received antiviral therapy (p=0.011).
Conclusions
UGI-CMV disease is not uncommon in immunocompetent patients, although symptoms are milder than those in immunocompromised patients. Our findings emphasize the importance of clinical vigilance for accurate diagnosis of CMV infection, particularly in susceptible symptomatic patients and highlight the need for active antiviral treatment for management of immunocompromised patients.
INTRODUCTION
Gastrointestinal (GI) cytomegalovirus (CMV) disease is a major contributor to mortality in immunocompromised patients [1]. Several recent descriptive case series have reported GICMV disease in immunocompetent hosts, and interest in CMV infection in this population has been increasing [2-6].
The prevalence of GI-CMV disease is approximately 5.0% in patients with AIDS [7]. Although the exact prevalence of CMV infection in immunocompetent patients remains unknown, CMV seroprevalence rates range between 40.0% and 100.0% in the adult population [7,8]. The overall unadjusted incidence rate of CMV end-organ disease in Korea was 0.52/100000 patients, and the overall CMV seropositivity rate in Koreans was estimated at 94.0% [9,10].
Few studies have investigated upper GI-CMV (UGI-CMV) disease, specifically in immunocompetent patients. Several retrospective studies have reported high mortality rates in patients with UGI-CMV disease [1,11]. However, these studies included a relatively small number of immunocompetent patients and enrolled patients with only CMV gastritis. Moreover, currently, no large-scale studies have investigated this condition, and diagnostic criteria and treatment guidelines for UGI-CMV disease remain unavailable [12,13].
In this study, we obtained data regarding UGI-CMV infection from five tertiary hospitals across the Honam province of Korea. We analyzed patient characteristics and diagnostic and therapeutic criteria in this patient population. We also compared the clinical characteristics and outcomes between immunocompromised and immunocompetent patients with UGI-CMV disease.
METHODS
Patient selection
This study performed between January 2010 and December 2022 included patients aged >17 years who were diagnosed with UGI-CMV disease. The five tertiary care Korean hospitals that participated in this study included Chonnam National University Hospital (1100 beds), Chonnam National University Hwasun Hospital (700 beds), Chosun University Hospital (850 beds), Jeonbuk National University Hospital (1100 beds), and Wonkwang University Hospital (810 beds).
The study was reviewed and approved by the Institutional Review Board (IRB) of Chonnam National University Hwasun Hospital (CNUHH-2023-171), Chonnam National University Hospital (CNUH-2023-360), and Jeonbuk National University Hospital (JBUH-2023-10-045). The requirement for informed consent was waived by the IRB owing to the retrospective study design.
Definitions
Patients were diagnosed with UGI-CMV disease if they met the following criteria: 1) clinical symptoms and signs such as nausea, vomiting, abdominal pain, dysphagia, or GI bleeding compatible with UGI tract infection, and 2) histopathologically confirmed CMV tissue infection documented by immunohistochemistry (IHC) or polymerase chain reaction (PCR) assays [14,15].
Confirmed GI-CMV disease was defined as a clinical presentation of GI disease in addition to CMV infection confirmed by IHC evaluation of biopsy specimens obtained from macroscopic lesions observed on endoscopy, without evidence of other pathogens [12,13].
Immunocompromised patients were defined as those with human immunodeficiency virus (HIV) infection, cancer (any solid or hematologic cancer regardless of a history of chemotherapy), a history of solid organ or stem cell transplantation, a history of steroid use over >4 weeks, or immunosuppressant use within 6 months preceding diagnosis. Immunocompetent patients were defined as healthy individuals without HIV infection, cancer, a history of steroid or immunosuppressant use within 6 months preceding study enrollment, or a history of solid organ or stem cell transplantation [6,16,17].
Treatment success was defined as resolution of patients’ symptoms or signs of GI disease, and recurrence was defined as recurrent UGI-CMV disease following successful treatment after an interval of at least 4 weeks during active surveillance [18,19].
Data collection
We retrospectively reviewed medical records and obtained patients’ demographic and clinical data. Comorbidities included hypertension, cardiovascular disease, diabetes mellitus, cerebrovascular disease, chronic kidney disease and/or end-stage renal disease that necessitated dialysis, rheumatological disease, neurological disease, liver disease (hepatitis and liver cirrhosis), pulmonary disease, solid tumors, and hematological malignancies. A history of chemotherapy, steroid use, blood transfusion, and antibiotic administration within 1 month of study enrollment were included as predisposing factors.
We also investigated patients regarding a history of selective histamine type 2 receptor blocker or proton pump inhibitor administration to determine the likely effect of these agents on the prevalence of UGI-CMV disease secondary to alterations in the intragastric environment [20,21]. Clinical data included symptoms of GI infection, time interval between symptom onset and diagnosis, endoscopic findings, as well as treatment and clinical outcomes.
Endoscopic findings were categorized as ulcers, erosions, exudates, polypoid and erythematous mucosa.
Diagnostic tools
IHC or PCR assays were used for histopathological confirmation of CMV tissue infection. CMV antibody clones (CCH2+DDG9, M0854; Dako, Glostrup, Denmark) were used for IHC evaluation, and a CMV QS-RGQ kit (Qiagen, Hilden, Germany) was used to perform PCR assays.
Statistical analysis
Patients’ baseline characteristics and clinical presentation are expressed as percentiles. Continuous variables were compared using the Student’s t-test or the Mann-Whitney U test. The χ2 and Fisher’s exact test were used to compare categorical variables. All p-values were two-tailed, and p-value <0.05 was considered statistically significant. The IBM SPSS for Windows software (version 20.0; IBM Corp., Armonk, NY, USA) was used for all statistical analyses.
RESULTS
Baseline characteristics and clinical presentation of patients with UGI-CMV disease
The study included 54 patients with UGI-CMV disease. Table 1 summarizes patients’ baseline characteristics, comorbidities, and clinical presentation.
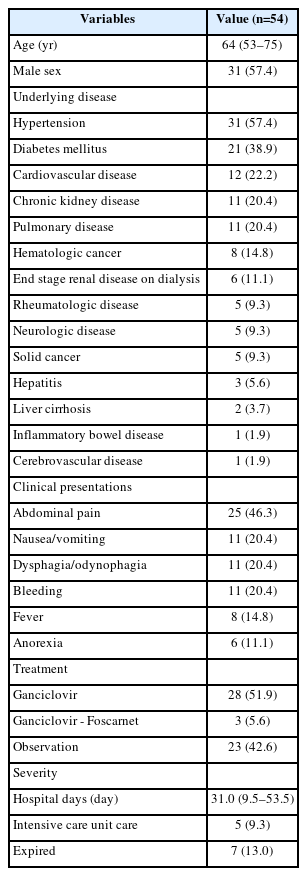
Baseline characteristics and clinical presentation of patients with upper gastrointestinal tract cytomegalovirus infection
The study population included 32 (59.3%) immunocompromised and 22 (40.7%) immunocompetent patients. Among the 32 immunocompromised patients, 10 had a history of solid organ transplantation, 8 had a history of hematological cancer (7 of 8 patients underwent stem cell transplantation), 5 had solid cancer, 5 received steroid therapy, 2 had HIV infection, and 2 patients received immunosuppressant therapy.
Patients’ median age was 64 years (interquartile range [IQR] 53–75 years), and 31 patients (57.4%) were males. The most common comorbidity was hypertension (57.4%), followed by diabetes mellitus (38.9%), cardiovascular diseases (22.2%), chronic kidney disease (20.4%), and pulmonary disease (20.4%).
The most common symptom associated with UGI-CMV disease was abdominal pain (46.3%), followed by nausea/vomiting (20.4%), dysphagia/odynophagia (20.4%), and bleeding (20.4%). Fever was observed in 8 patients (14.8%).
Endoscopic findings of patients with UGI-CMV disease
Among 54 patients, 27 (50.0%) had UGI-CMV infection of the esophagus, 24 (44.4%) had gastric involvement, and 3 patients (5.6%) showed duodenal disease. The most common endoscopic findings of UGI-CMV disease were ulcers (70.4%), followed by erythematous mucosa (44.4%), erosions (24.1%), exudates (16.7%), and polypoid mucosal lesions (7.4%). Table 2 shows endoscopic findings based on the site of involvement.
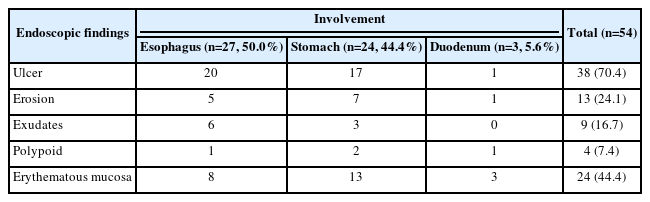
Endoscopic findings based on the site of invasion in patients with upper gastrointestinal tract cytomegalovirus infection
Treatment and prognosis of patients with UGI-CMV disease
Antiviral treatment was administered to 31 patients (57.4%, median duration 21.0 days); however, 23 patients (42.6%) did not receive antiviral treatment. Among the 31 patients who received antiviral treatment, ganciclovir was administered to 28 patients (51.9%), and 3 patients (5.6%) received foscarnet as second-line therapy.
The median length of hospitalization was 31.0 days (IQR 9.5–53.5 days), and 5 patients (9.3%) required intensive care unit (ICU) admission.
Of the 7 patients (13.0%) who died in this study, only one patient died of UGI-CMV disease-related causes. This patient showed multi-organ involvement, including the esophagus, stomach, and duodenum, and death was attributable to severe recurrent bleeding from a duodenal ulcer. The other 6 patients died of intracranial hemorrhage, graft-versus-host disease (GVHD) and hospital-acquired pneumonia (Table 1).
Comparison between immunocompromised and immunocompetent patients with UGI-CMV disease
Baseline characteristics and underlying comorbidities
Immunocompetent patients were older (median age 68.7 years vs. 55.8 years) and less likely to be male (40.9% vs. 68.8%) compared with immunocompromised patients. No significant intergroup differences were observed in underlying comorbidities. However, acid suppressant use (75.0% vs. 45.5%, p=0.027), a history of recent transfusion (43.8% vs. 13.6%, p=0.019), and history of recent antibiotic use (71.9% vs. 31.8%, p=0.004) were more frequent in immunocompromised than in immunocompetent patients. No significant intergroup difference was observed in laboratory and endoscopic findings (Table 3).
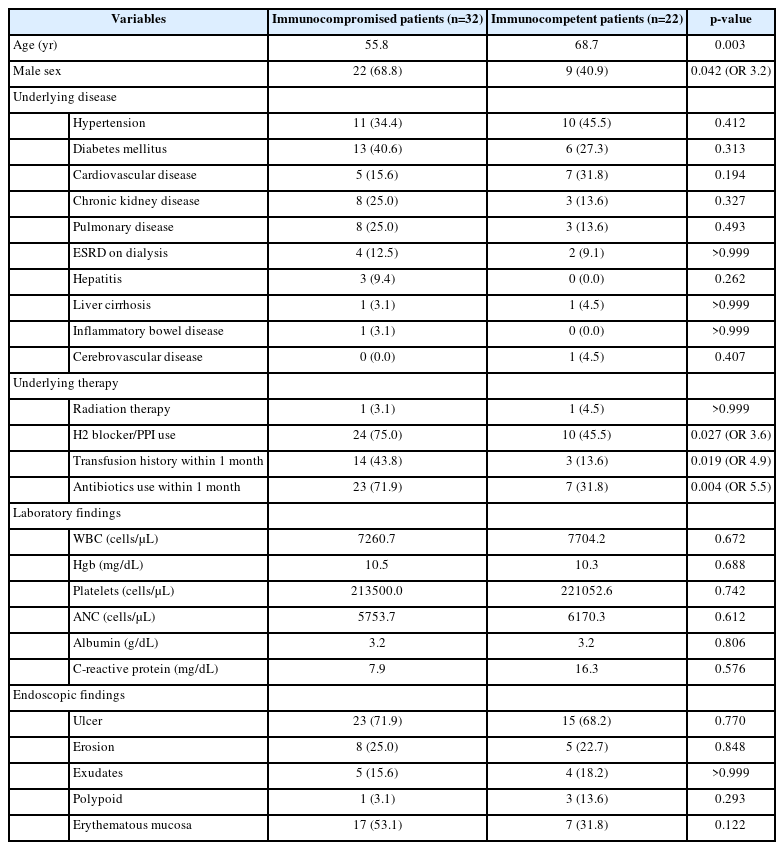
Comparison of baseline characteristics and comorbidities between immunocompromised and immunocompetent patients
Treatment outcomes
The rate of antiviral treatment was higher among immunocompromised patients (24 patients, 75.0%) than among immunocompetent patients (7 patients, 31.8%). Among immunocompromised patients, 8 patients (25.0%) did not receive antiviral therapy, which was attributable to the following factors: mild symptoms (5 patients), treatment rendered for other diseases (e.g., GVHD, 2 patients), and death before the results of the CMV test were available (1 patient).
Among immunocompetent patients, observation without treatment was attributable to the following factors: mild symptoms (10 patients), concurrent treatment for other diseases (e.g., Behçet’s disease, 3 patients), death before the results of the CMV test were available (1 patient), and voluntary discharge (1 patient).
The median duration of admission was longer in immunocompromised patients (46.2 vs. 20.0 days, p=0.001). However, no significant intergroup differences were observed in treatment success rates, as well as in ICU admission and mortality rates (Table 4).
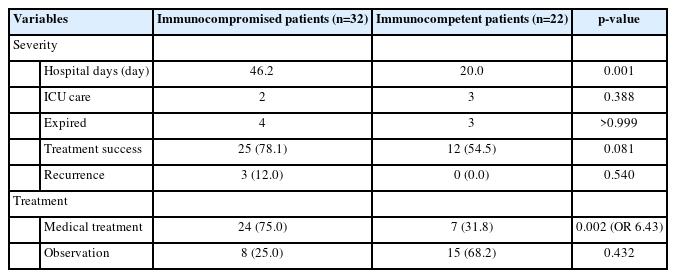
Comparison of treatment outcomes between immunocompromised and immunocompetent patients
Comparison of treatment outcomes based on antiviral therapy in immunocompromised and immunocompetent patients
Table 5 illustrates the length of hospitalization, ICU admission, mortality, and recurrence rates in immunocompromised and immunocompetent patients based on administration of antiviral therapy.

Comparison of treatment outcomes between immunocompromised and immunocompetent patients with regard to antiviral therapy
Among immunocompromised patients, those who received antiviral therapy had a median length of hospitalization of 43.0 days compared with 23.5 days in those who did not receive antiviral therapy. Among patients who received antiviral therapy, 2 (8.3%) required ICU admission; however, both patients eventually died, and 2 patients (25.0%) from the untreated patient group died. Recurrent UGI-CMV disease occurred in 12.5% of patients who received antiviral therapy; however, no recurrence was observed in patients who underwent observation. Among immunocompetent patients, those who received antiviral therapy had a median length of hospitalization of 31.0 days vs. 7.0 days in patients who did not receive antiviral therapy. ICU admission and mortality rates were comparable between patients who did and did not receive antiviral therapy. No recurrence was observed in immunocompetent patients. Statistical analysis revealed no significant differences in length of hospitalization, ICU admission, and recurrence based on administration of antiviral therapy in either group.
Table 6 illustrates treatment success rates among immunocompromised and immunocompetent patients based on antiviral therapy. Among the immunocompromised patients, 87.5% were successfully treated using antiviral therapy, compared with 50.0% who did not receive this treatment, and this difference was statistically significant (p=0.011). Among immunocompetent patients, 85.7% and 40.0% were successfully treated with and without antiviral therapy, respectively; however, this difference was statistically insignificant. In the subgroup of 15 immunocompetent patients who did not receive antiviral treatment, 6 were treated successfully, whereas the remaining 9 patients were lost to follow-up or were voluntarily discharged; therefore, their status remains unknown.

Comparison of treatment success rates of antiviral therapy between immunocompromised and immunocompetent patients
DISCUSSION
Human CMV, a member of the Herpesviridae family, is a double-stranded DNA virus. CMV infection is prevalent worldwide and is associated with a wide spectrum of diseases depending on the host immune status [22,23]. Transmission of infection usually occurs via exposure to body fluids, including saliva, blood, or semen through close contact with infected adults [24]. Asymptomatic infections are common with specific immunoglobulin G antibodies detected in patients’ serum (approximately 60.0% in developed and >90.0% in many developing countries) [25].
Host immunity is a major determinant of the clinical manifestations of CMV infection. Following primary infection, CMV establishes a state of latency secondary to an initial immune response in an immunocompetent host. Few primary CMV infections in immunocompetent patients produce symptoms; however, CMV infection in immunocompromised patients leads to systemic disease with severe complications and a high mortality rate [26].
GI-CMV infections involve the esophagus, stomach, small bowel, colon, and liver; the colon is most commonly affected. Severely immunocompromised patients usually develop tissueinvasive CMV infection characterized by symptoms and endoscopic abnormalities [6]. However, as observed in our study, relative immunosuppression that occurs during periods of critical illness or in patients with comorbidities, may increase susceptibility to CMV in immunocompetent patients [6,27]. Therefore, although categorized as immunocompetent, aged patients and those with comorbidities show an immune-deficient status of varying degrees and may have reactivation or primary CMV infection with a clinical presentation of CMV infection.
Diagnosis of UGI-CMV infection is largely based on IHC of tissue samples and tissue-specific PCR analysis [28]. Tissue IHC staining is accepted as the gold standard for GI-CMV disease, with sensitivity and specificity of 93.0%–100.0% and 91.0%– 93.0%, respectively. Sensitivity (33.0%–100.0%) and specificity (60.0%–89.0%) of tissue CMV DNA PCR was lower than that of IHC [29-31].
Endoscopic findings of CMV infection vary, with ulcerative lesions being the most prevalent in our study. Superficial mucosal changes, such as erythema and erosion, were the second most frequent findings. No intergroup differences were observed in endoscopic characteristics.
The clinical characteristics of the immunocompromised and immunocompetent groups did not differ in our study, except for older age of members in the immunocompetent group. Compared with immunocompetent patients, immunocompromised patients had more frequent acid suppressant use, recent transfusion history, and recent antibiotic use. However, these differences are not attributable to CMV disease but to the underlying conditions associated with immunodeficiency in these patients. These findings are consistent with those published previously; however, further large-scale cohort studies are warranted for clarification [17,32-34].
We observed that in both the immunocompromised and immunocompetent groups, length of hospitalization was longer in patients who received antiviral therapy than in those who did not receive this treatment. It is difficult to definitively attribute this finding to the effect of antiviral therapy itself, because these drugs were predominantly administered to patients with comorbidities and more severe symptoms. We concluded that antiviral therapy was administered to patients with a more severe clinical presentation, whereas the expectant observation approach was adopted in patients with subclinical symptoms not attributable to the CMV infection itself. Although we observed no statistically significant intergroup differences in treatment success rates, it is likely that many patients in the immunocompetent group (9 patients) were voluntarily discharged or were lost to follow-up, which may have potentially affected accurate estimation of treatment success rates.
Among immunocompromised patients, the treatment success rate was higher following antiviral treatment, which suggests the importance of active antiviral drug use in this population. A high percentage of patients in the immunocompetent group underwent observation without antiviral therapy, and no recurrence was observed in any patient regardless of antiviral therapy. Therefore, even after tissue-based diagnosis of CMV in immunocompetent patients, it is challenging to conclusively establish significant CMV disease, which is possibly attributable to the high natural remission rate of CMV or the detection of innocent bystander CMV.
Fatality and ICU admission rates were primarily associated with the severity of underlying diseases and not the etiology of UGI-CMV disease in both immunocompromised and immunocompetent patients.
In conclusion, our 10-year multicenter retrospective study based on data obtained from tertiary medical centers across Korea was larger than previous studies that have discussed this subject. CMV infection is prevalent in the general population; however, clinically significant tissue-invasive UGI-CMV infections are rare and diagnostically challenging. Previously, CMV infection was considered a disease only in immunocompromised patients. Owing to its ubiquitous nature, CMV infection in its latent period is common. CMV infection may occur even in relatively healthy immunocompetent individuals, as observed in our study. Aged patients, those with comorbidities, or those with critical illness are susceptible to tissue-invasive CMV infection, although clinical outcomes are milder in this patient population compared with those in immunocompromised patients. Therefore, clinicians should be alert regarding diagnosis of endoscopically detected lesions with a high index of clinical suspicion for CMV infection in susceptible symptomatic patients.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors have no financial conflicts of interest.
Funding Statement
None
Authors’ Contribution
Conceptualization: Ga-ram You, Wan-sik Lee. Data Curation: Ga-ram You, Seon-young Park, Hye-su You, Seung-young Seo, Sung-kyun Yim, Byung-chul Jin, Jung-in Lee, Young-dae Kim, Suck-chei Choi, Chan- Guk Park. Formal Analysis: Ga-ram You, Seon-young Park, Hye-su You, Seung-young Seo, Sung-kyun Yim, Byung-chul Jin, Jung-in Lee, Young-dae Kim, Suck-chei Choi, Chan-guk Park. Investigation: Ga- Ram You, Wan-sik Lee. Methodology: Ga-ram You, Wan-sik Lee. Project Administration: Wan-sik Lee. Resources: Ga-ram You. Software: Ga-ram You. Supervision: Wan-sik Lee. Validation: Ga-ram You. Visualization: Ga-ram You. Writing—original Draft: Ga-ram You. Writing— Review & Editing: Ga-ram You, Wan-sik Lee. Approval Of Final Manuscript: All Authors.
Acknowledgements
None