위염의 교토 분류와 개정된 시드니 체계 간의 연관성
Association between the Kyoto Classification of Gastritis and the Updated Sydney System
Article information

Article: Consistency between the endoscopic Kyoto classification and pathological updated Sydney system for gastritis: a cross-sectional study (J Gastroenterol Hepatol 2022;37:291-300)
요약: 위염을 진단하기 위해 서양에서는 전정부의 소만과 대만, 체부의 소만과 대만, 위각에서 각각 조직 검사를 하도록 권하고 있으나[1], 정기적인 위내시경 검진을 하는 우리나라와 일본에서는 검사할 때마다 여러 부위에서 조직 검사를 반복하기는 어렵다. 위 단면 연구에서는 서양의 조직 검사 기준을 대체할 수 있는 위염의 내시경 소견을 제시하고자 개정된 시드니 체계(updated Sydney system) 점수와 위염의 교토 분류(Kyoto classification for gastritis) 점수 간의 연관성을 비교 분석하였다[2]. 연구 대상은 헬리코박터 파일로리(Helicobacter pylori, H. pylori) 검사를 처음 받는 일본인 721명(평균 나이 49.2세, 여성의 비율 57.8%)이었다.
조직 검사 소견은 시드니 체계에 준하여 호중구, 단핵구, 위축, 장상피화생, H. pylori에 대해 각각 0~3점(none, mild, moderate, marked)으로 채점하였다[3]. H. pylori 감염은 조직 검사에서 균이 관찰되거나 요소호기 검사에서 양성 소견을 보이면 진단하였다. 한편, 조직 검사에서 음성 소견을 보이고 요소호기 검사와 혈청 E-plate Eiken H. pylori antibody II (Eiken Chemical, Tokyo, Japan) IgG 수치가 <10 U/mL로 음성 소견을 보이면 감염이 없다고 진단하였다. 조직 검사와 혈청 검사 결과가 다른 경우에는 요소호기 검사로 감염 여부를 판단하였다. 그 결과, 721명 중 450명이 H. pylori 감염자로 분류되었다.
위내시경 소견은 교토 분류의 5대 전암성 병변인 위축, 장상피화생, 주름 비대, 결절, 광범위한 발적에 대해 조사하였다[4]. 위축이 없거나 위축 경계가 전정부에서 보이는 폐쇄형 I형 위축성 위염이면 0점, 위축 경계가 체부의 소만에서 관찰되는 폐쇄형 위축 II형이나 III형이면 1점, 위축 경계가 분문부를 침범한 개방형 위축이면 2점으로 채점하였다. 장상피화생은 전정부에서만 보이면 1점, 체부에서도 보이면 2점으로 채점하였다. 주름 비대는 5 mm 이상의 위주름이 보이면 1점, 결절은 전정부에서 닭살 모양이 보이면 1점으로 채점하였다. 광범위한 발적이 체부와 기저부에서 약하게 보이거나 부분적으로 정상 혈관상(regular arrangement of collecting venules)이 보이면 1점, 발적이 심하고 정상 혈관상이 보이지 않으면 2점으로 채점하였다.
그 결과, 체부 조직 검사에서 호중구와 단핵구 침윤이 있으면 위내시경에서 광범위한 발적, 주름 비대, 결절이 관찰될 가능성이 높았다. 한편, 위내시경에서 위축 점수가 높을수록 체부 조직 검사에서 위축과 장상피화생 점수가 높았으며, 위내시경에서 장상피화생 점수가 높을수록 전정부와 체부 조직 검사에서 위축과 장상피화생 점수가 높았다. 결론적으로, 위염의 교토 분류 점수는 병리 소견을 반영하므로, 위내시경 검사 시 주름 비대, 결절, 광범위한 발적 및 위축과 장상피화생의 범위를 제대로 진단할 수 있다면 매번 조직 검사를 하지 않아도 될 것이다.
해설: H. pylori 균이 발견된 후, 지난 40년간 위염을 진단하는 다양한 방법들이 개발되었다. 서양에서 중요시하는 Operative Link for Gastritis Assessment (OLGA)와 Operative Link for Gastric Intestinal Metaplasia Assessment (OLGIM)는 위축이나 장상피화생에서 발생하는 느린 장형 위암을 예측할 수 있지만[5], 위축이나 장상피화생 없이 발생하는 미만형 위암은 예측하지 못한다. 특히 우리나라에는 동아시아형 cytotoxin-associated gene A (CagA) 독성인자를 지닌 H. pylori 균에 의한 감염이 흔한데[6], 위축이나 장상피화생 없이 미만형 위암이 발생할 경우에는 OLGA나 OLGIM 점수가 도움이 안 된다. 이에 이 연구에서는 동아시아형 CagA를 지닌 H. pylori 감염 시 흔히 관찰되는 내시경 소견을 중심으로 시드니 분류 체계 점수와의 연관성을 분석하였다[2]. 그 결과, 주름 비대, 결절, 광범위한 발적이 관찰되면 체부 조직 검사에서 높은 호중구와 단핵구 침윤 점수를 보였으며, 전정부의 조직 검사에서 낮은 위축과 장상피화생 점수를 보였다.
이 연구가 중요한 이유는 OLGA나 OLGIM 점수로는 예측할 수 없는 위암의 위험성을 주름 비대, 결절, 광범위한 발적으로 입증하였기 때문이다[2]. 광범위한 발적은 H. pylori 균에 의한 급성 염증으로 인해 상피하 모세혈관이 충혈되고 확장될 때 보인다[7]. 주름 비대는 H. pylori 감염이 고가스트린혈증을 유발할 때 관찰되며, 변형된 벽세포와 긴 선와상피세포로 구성된다[8]. 결절은 H. pylori 감염으로 인해 점막하층에 모인 림프 여포(lymphoid follicle)와 림프 혈장계 세포의 응집(lymphoplasma cell aggregate)으로 구성되는데, 제균하지 않으면 위축성 위염이나 화생성 위염으로 변해간다[9]. 이 세 가지 소견은 혈청 항H. pylori IgG 수치와 비례하였으며[7,8,10], 체부에서 호중구와 단핵구 침윤 점수가 높고 전정부에서 위축과 장상피화생 점수가 낮을수록 흔하게 관찰되었다[2,11].
이러한 동서양 간의 차이를 감안하여 이 연구에서는 서양 연구에서 등한시하는 급성 활동성 감염 시의 위염에 대한 소견을 강조하였다[2]. 위암 발생의 주요 원인을 숙주 요인으로 보는 서양과 달리 우리나라와 일본에서는 균주 요인이 중요하다[12]. 서양에서는 미만형 위암의 원인을 E-cadherin 1 (CDH1) 변이가 관찰되는 희귀한 유전 질환(hereditary diffuse gastric carcinoma)으로 해석하는 경향이 있으나, 우리나라에서는 동아시아형 CagA를 지닌 H. pylori 균에만 감염되어도 CDH1 변이가 흔히 관찰된다[13]. 그리고 이때 발생하는 미만형 위암은 주름 근처에서 호발하며, 체부에 호중구와 단핵구 침윤이 심하고 광범 위한 발적이나 주름 비대 또는 결절이 흔히 보인다(Table 1). 활동성 감염 시 내시경으로 관찰되는 광범위한 발적, 주름 비대, 결절이 시드니 체계에서 위축이나 장상피화생 점수가 낮을수록 흔하다는 이번 연구 결과가 이를 뒷받침한다[2]. 국내 연구에서도 미만형 조기위암은 높은 혈청 항H. pylori 항체 수치와 연관되어 활동성 감염자에서 미만형 위암이 발생할 위험성이 높다는 것을 보여주었다[14].
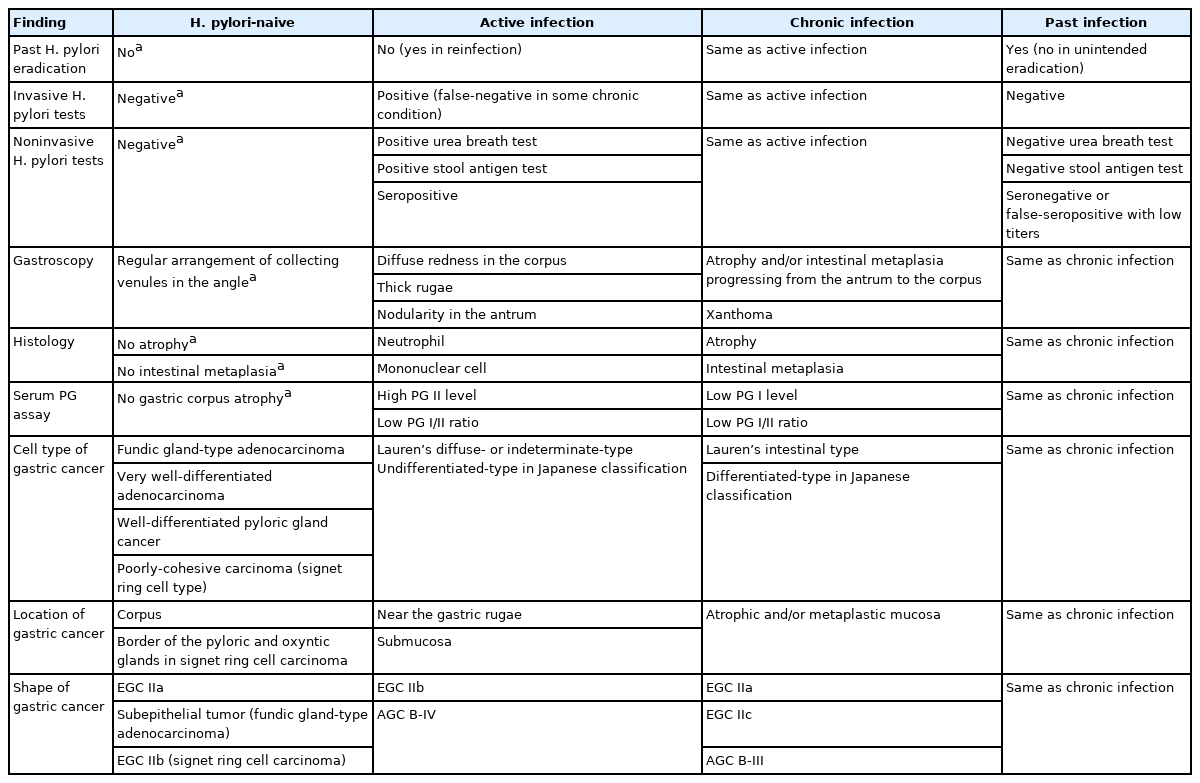
Common Findings Observed in Koreans According to the Infection Status of Helicobacter pylori
향후 필요한 연구는 H. pylori에 감염된 적이 없는 위에서 발생하는 위염의 내시경 소견과 조직 검사 소견에 대한 분석이다. 이번 연구에서는 H. pylori 음성으로 진단된 사람이 271명(37.6%)에 불과하고, 미감염자와 과거 감염자를 구분하지 않아서 교토 분류 점수가 전정부와 체부의 단핵구 침윤과 비례하는 비특이적인 소견을 보였다[2]. 또한, 광범위한 발적, 주름 비대, 결절, 위축, 장상피화생으로 구성된 5대 전암성 내시경 소견 이외에 교토 분류의 다른 내시경 소견들[15]에 대해서는 분석하지 않았다는 한계점이 있다. 우리나라에서도 미감염자가 증가하고 있다는 점과 미감염자에서 발생하는 위암의 특징들을 고려할 때[16], 한국인 미감염자에게 위암을 유발할 수 있는 위염에 대한 내시경 소견과 조직 검사 소견을 분석하여 현 감염자 및 과거 감염자들과 감별하려는 노력이 필요하다.
Notes
No potential conflict of interest relevant to this article was reported.