무증상 저나트륨혈증을 동반한 식도 종괴
Esophageal Mass With Asymptomatic Hyponatremia
Article information

요 약
62세 남자가 고립성 폐결절로 주기적인 흉부 전산화 단층촬영 추적 관찰 중 흉강내 림프절들의 크기 증가로 평가를 위해 호흡기 내과로 입원하였다. 다른 기저 질환은 없었다. 입원시 시행한 혈액 검사에서 혈청 나트륨 111 mmol/L로 저하되어 있었으나 특별한 증상은 없었고 다른 혈액검사들은 이상 소견이 없었다. 조영 증강으로 복부, 흉부 전산화 단층촬영을 다시 시행하였고 흉강내, 좌측 쇄골상 림프절 크기 증가와 더불어 하부 식도 벽의 비후와 복강내 림프절 크기 증가도 관찰되었다. 양전자 방출 단층촬영에서 같은 위치들에 악성이 의심되는 흡수 증가 소견들이 보였다(Fig. 1). 소화기내과로 의뢰되어 상부위장관 내시경 검사를 시행하였고 하부 식도에 5 cm 길이의 궤양성 종괴가 관찰되었다(Fig. 2). 의심되는 진단은 무엇인가?

Radiologic findings of the patient. A and B: Chest computed tomography (CT) shows enlarged left supraclavicular lymph node and mediastinal lymph node. C: Esophageal wall thickening was revealed on chest CT (arrows). D: Enlarged abdominal lymph node was seen in CT. E and F: Positron emission tomography reveals uptake suspected of malignancy on the same locations as in the CT.
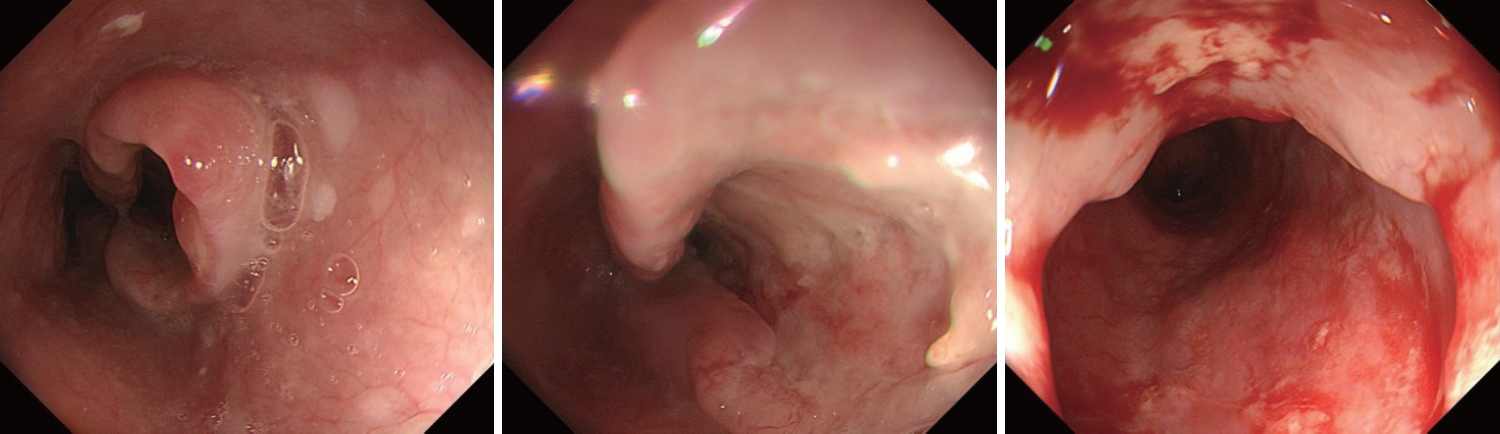
A 5 cm-sized, ulcerative mass on lower esophagus was observed in endoscopy.
해 설
식도 종괴에 대한 내시경 조직 검사를 시행하였다. 조직 검사에서 세포질이 거의 없는 작은 원형의 악성 세포들이 관찰되었고 면역화학염색에서 panCK, TTF-1, CD56 양성 소견으로 소세포암종(small cell carcinoma)으로 진단할 수 있었다(Fig. 3). 환자는 흉강 내, 복강내 림프절 전이를 동반한 식도 소세포 암으로 최종 진단되었다. 확장 병기의 소세포암으로 Etoposide와 Cisplatin 조합의 전신 항암치료를 시작하였고 저나트륨혈증은 2차 항암 치료를 위해 입원하였을 때 혈청 나트륨 수치가 124 mmol/L로 상승되었고, 3차 항암 치료부터는 정상으로 회복되었다. 항암치료를 지속하며 시행한 추적 검사에서 림프절 전이들의 크기가 감소하고 식도 궤양성 종괴도 호전 소견을 보였다(Fig. 4).
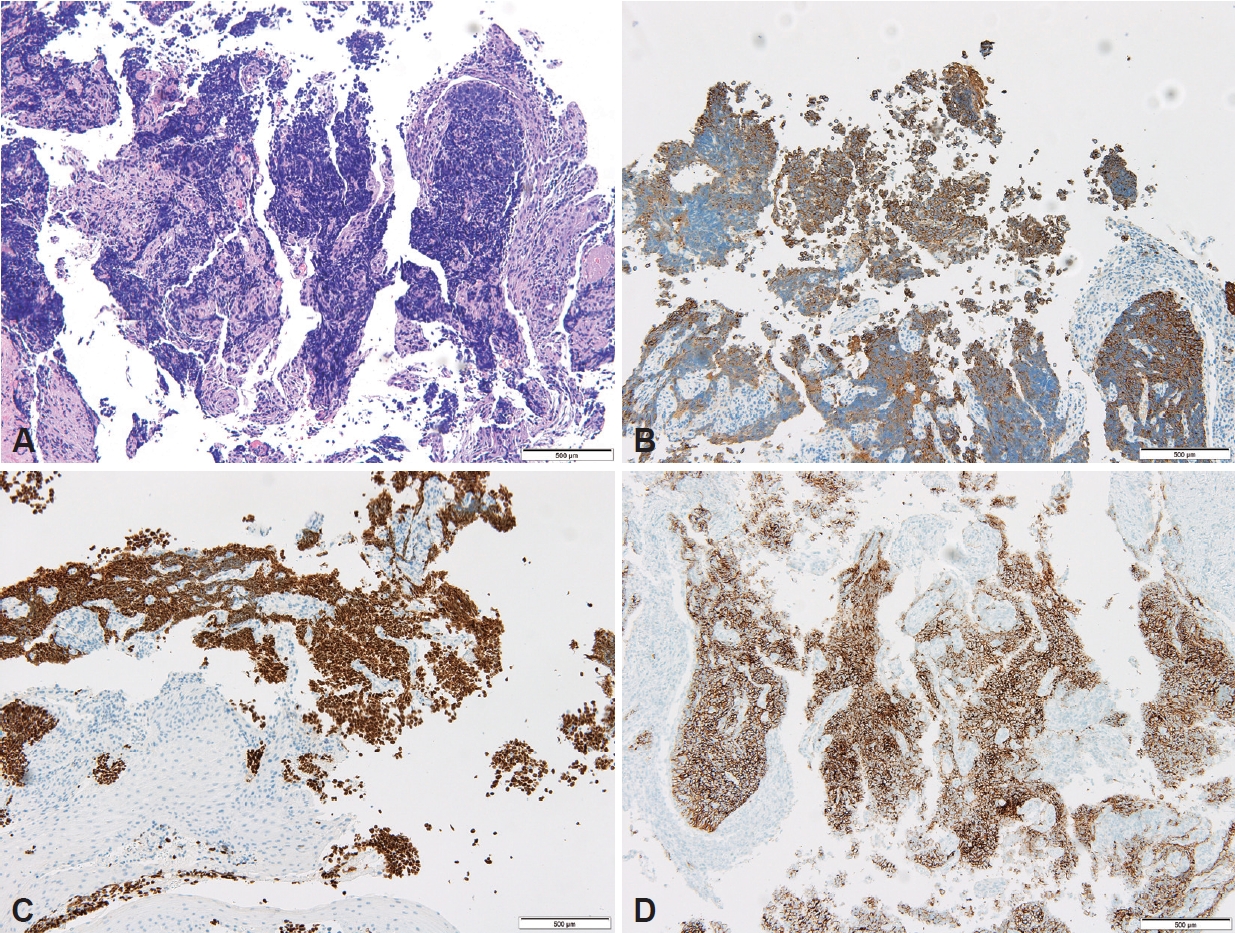
Pathologic findings of the biopsy. A: Small round tumor cells containing scant cytoplasm were observed (H&E stain, ×100). B-D: The cells showed immunohistochemical positivity for panCK, TTF-1, and CD56 (×100). Scale bars=500 μm. H&E, hematoxylin and eosin.

The esophageal mass had improved in endoscopy after six cycles of chemotherapy.
식도 소세포암은 전체 식도암의 0.8%-2.4%로 매우 드물지만 폐외 소세포암 중에는 식도가 가장 호발 부위이다[1,2]. 식도 소세포암은 예후가 매우 좋지 않아 5년 생존율은 6%-7% 정도 밖에 되지 않는다[3]. 치료는 폐 소세포암과 비슷하게 제한 병기에는 수술이나 동시 항암방사선 치료를, 확장 병기에는 전신 항암치료를 할 수 있다[3].
소세포암은 다른 암들에 비해 암세포에서 분비하는 호르몬에 의한 부종양증후군(paraneoplastic syndrome)이 흔하게 발생할 수 있으며 그 중 항이뇨호르몬이 부적절하게 분비되어(syndrome of inappropriate antidiuretic hormone, SIADH) 저나트륨혈증이 발생할 수 있다[4]. 소페포암에서 발생한 SIADH로 인한 저나트륨혈증은 대부분 암에 대한 치료가 되면 호전되며 실제 소세포 폐암 환자들의 저나트륨혈증은 항암치료를 시작하면 수 주 이내 호전되는 것으로 알려져 있다[5].
Notes
Availability of Data and Material
Data sharing not applicable to this article as no datasets were generated or analyzed during the study.
Conflicts of Interest
Dae Gon Ryu, a contributing editor of The Korean Journal of Helicobacter and Upper Gastrointestinal Research, was not involved in the editorial evaluation or decision to publish this article.
All remaining authors have declared no conflicts of interest.
Funding Statement
This study was supported by a 2023 research grant from Pusan National University Yangsan Hospital.
Authors’ Contribution
Conceptualization: Cheol Woong Choi. Data curation: Dae Gon Ryu. Formal analysis: Dae Gon Ryu. Funding acquisition: Dae Gon Ryu. Investigation: Dae Gon Ryu. Methodology: Dae Gon Ryu. Project administration: Dae Gon Ryu. Resources: Dae Gon Ryu. Software: Dae Gon Ryu. Supervision: Cheol Woong Choi. Validation: Dae Gon Ryu. Visualization: Dae Gon Ryu. Writing—original draft: Dae Gon Ryu. Writing—review & editing: Dae Gon Ryu. Approval of final manuscript: all authors.
Acknowledgements
None.