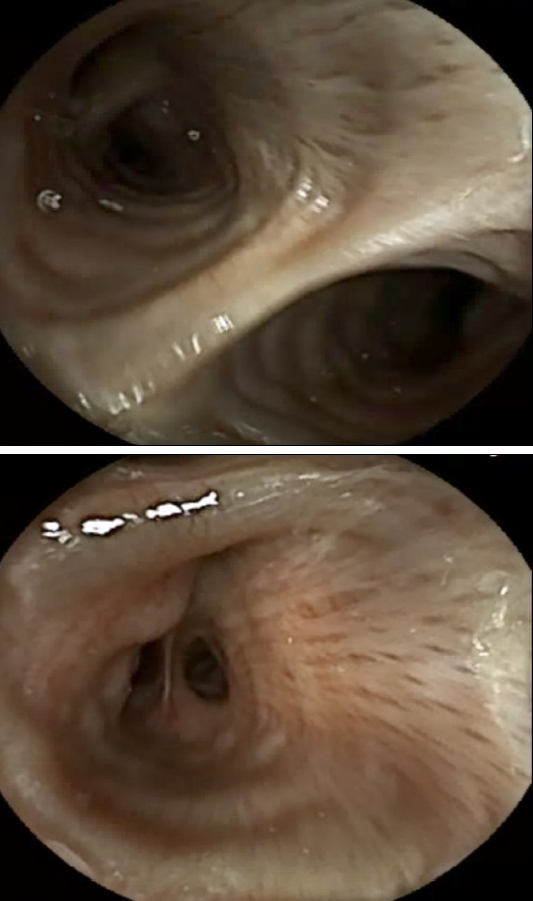
Question: An 82-year-old man presented with melena and anemia. There were no other symptoms, such as abdominal pain or weight loss. He had hypertension, atrial fibrillation, and mild aortic regurgitation, and was taking medication, including an anticoagulant. There was no history of cerebrovascular or neurological disorders. He denied any alcohol consumption or smoking. Laboratory tests showed a serum hemoglobin level of 9.1 milligrams per deciliter, a serum ferritin level of 13.26 micrograms per deciliter, and a serum iron saturation below 10 percent. The fecal occult blood test was positive. Esophagogastroduodenoscopy and sigmoidoscopy did not reveal any gastrointestinal bleeding, and abdominal computed tomography also demonstrated no evidence of an active bleeding focus. A video capsule endoscopy (CE) using PillCam SB 3 system (Medtronic, Minneapolis, MN, USA) was performed to examine small bowel bleeding. Before the procedure, the patient was evaluated with neurological examinations to exclude oropharyngeal dysphagia, and he did not show any abnormal findings. Under the supervision of a physician, the patient swallowed the CE. Immediately after swallowing, he experienced a cough and a foreign body sensation in the thorax. Vital signs were stable. Subsequently, 47 seconds after the start of recording, the real-time images of CE revealed a bifurcated lumen (Fig. 1). What is the most likely diagnosis?
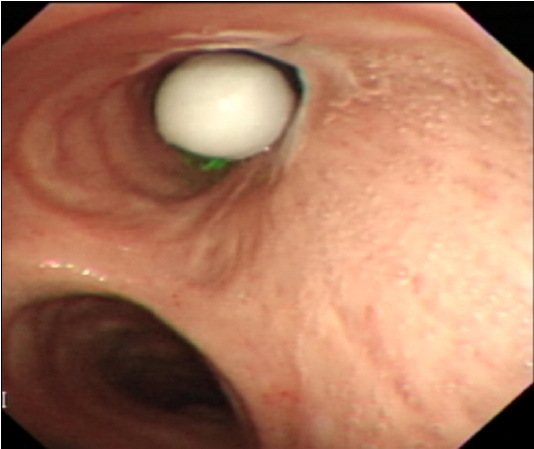
Answer: After swallowing the CE, the patient kept complaining of chest discomfort without any respiratory distress. However, the real-time images of the CE revealed a bifurcated lumen with ring-shaped cartilage branching multiple times (Fig. 1), raising suspicion of capsule aspiration. Flexible bronchoscopy was performed urgently, confirming the presence of the CE impacted in the right main bronchus (Fig. 2). The capsule was subsequently removed using a snare. There were no complications after the procedure, and the post-procedure chest X-ray was normal. The entire duration of CE aspiration was approximately one hour.
Since its introduction in 2001, video CE has been widely used for evaluating inflammatory bowel disease, obscure gastrointestinal bleeding, and iron-deficiency anemia [1]. The overall complication rate is approximately 1~3%, making it a safe procedure [2]. Various complications have been reported, including retenton, swallow failure, aspiration, incomplete examination, and technical failure; the most commonly reported complication is capsule retention, especially in patients with inflammatory bowel disease [3].
Capsule aspiration is defined as the aspiration of the CE into the airway during the swallowing process and was first reported by Schneider et al. in 2003 [4]. Although capsule aspiration is rare, occurring in about 0.1% of investigations, it can lead to life-threatening consequences such as respiratory failure and obstructive pneumonitis [3]. A systematic review by Yung et al. [2] revealed that approximately 40% of cases showed no symptoms, and if any symptoms were present, they were typically mild, indicating a low occurrence of severe respiratory complications. In our case, the patient also experienced only a cough and chest discomfort without severe respiratory symptoms, such as desaturation or dyspnea.
Individuals who are elderly or have neurologic deficits are considered a high-risk group for capsule aspiration [5]. However, 90% of CE aspiration cases were without history of dysphagia [2]. Therefore, caution is needed not only when examining high-risk patients, but also when examining patients with normal neurological examinations. Particularly, even if severe respiratory symptoms are not presented after the examination, there is still a possibility of asymptomatic aspiration, necessitating the use of real-time imaging of CE or a plan X-ray for localization of the CE after the procedure. Additionally, direct endoscopic delivery of CE into the gastrointestinal tract may also be helpful in these patients. If capsule aspiration is confirmed, inducing cough or attempting maneuvers like back blowing could be considered as first-line management because coughing up the capsule can lead to spontaneous resolution of capsule aspiration [2]. However, if the aspiration is refractory, prompt bronchoscopic removal should be considered.