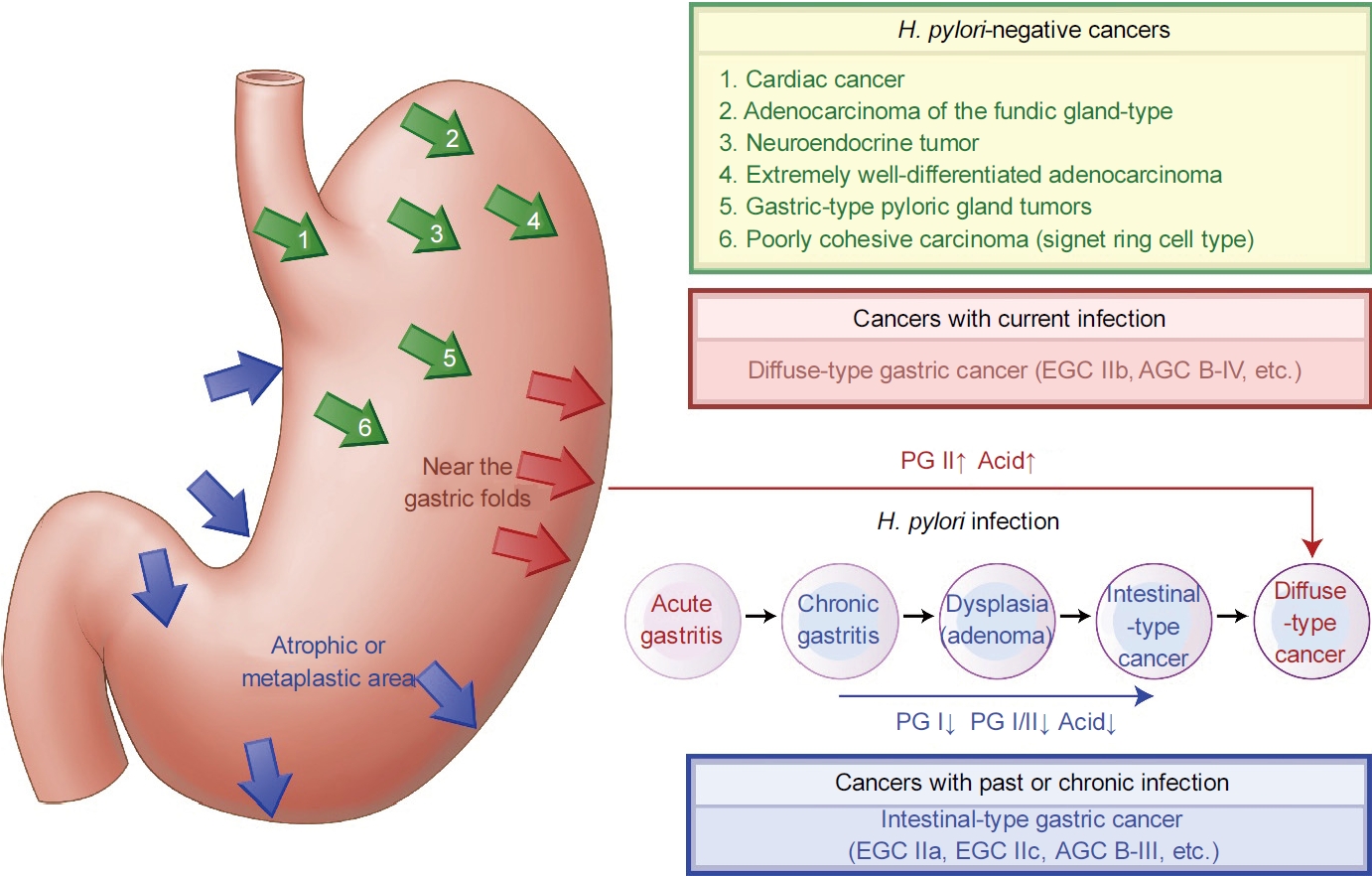
The National Cancer Screening Program still recommends biennial gastric cancer screening to all Koreans aged between 40 and 74 years [1]. A total of 6,916,632 (55.7%) Koreans underwent gastric cancer screening among the target population of 12,409,918 in 2020 [2]. According to the data, most (90.8%) underwent gastroscopy in 2020. Only 9.2% underwent upper gastrointestinal series (UGIS). Although endoscopic screening decreased gastric cancer-related mortality in Koreans [3], the current strategy needs to be revised for the following reasons. First, the age-standardized incidence rate of gastric cancer has decreased by 4.6% per year since 2011, reaching 30.4 per 100,000 population in 2019 [4]. Second, the prevalence of Helicobacter pylori (H. pylori)-seropositivity is decreasing [5]. It was 74.3% in 1990, but decreased to 43.9% in 2016. Third, among seronegative subjects, past infection is common only in elderly Koreans born before 1960 [6]. In other words, H. pylori-naive stomachs are common in the younger population born thereafter. Lastly, the type and location of gastric cancers differ between H. pylori-infected, -eradicated, and -naive individuals (Fig. 1). Hence, different strategies should be considered instead of performing biennial gastroscopy in all Koreans aged ≥40.
Besides gastroscopy and UGIS, several methods have been suggested for gastric cancer screening. Nonetheless, no large-sized studies have reported significant decreases in gastric cancer-related mortality in Koreans, except for studies using gastroscopy. Non-invasive H. pylori tests, including the serology test, are also mentioned; however, these tests cannot diagnose gastric cancer itself. Similarly, a combination of serology titers and serum pepsinogen (PG) tests cannot detect gastric cancer, but it helps detecting high-risk individuals for gastric cancers and adenomas [7]. Low PG I/II ratios indicate an increased risk for gastric adenoma and intestinal-type cancer, and high PG II levels indicate that for diffuse-type gastric cancer [8]. Furthermore, a low PG I/II ratio and a high PG II level help discriminate current H. pylori infection [9]. The study showed that low PG I/II ratios below 4.35 and high PG II levels over 12.95 ng/mL correlated with a positive urea breath test (UBT) finding in asymptomatic Koreans (sensitivity: 91.6%, specificity: 94.3%).
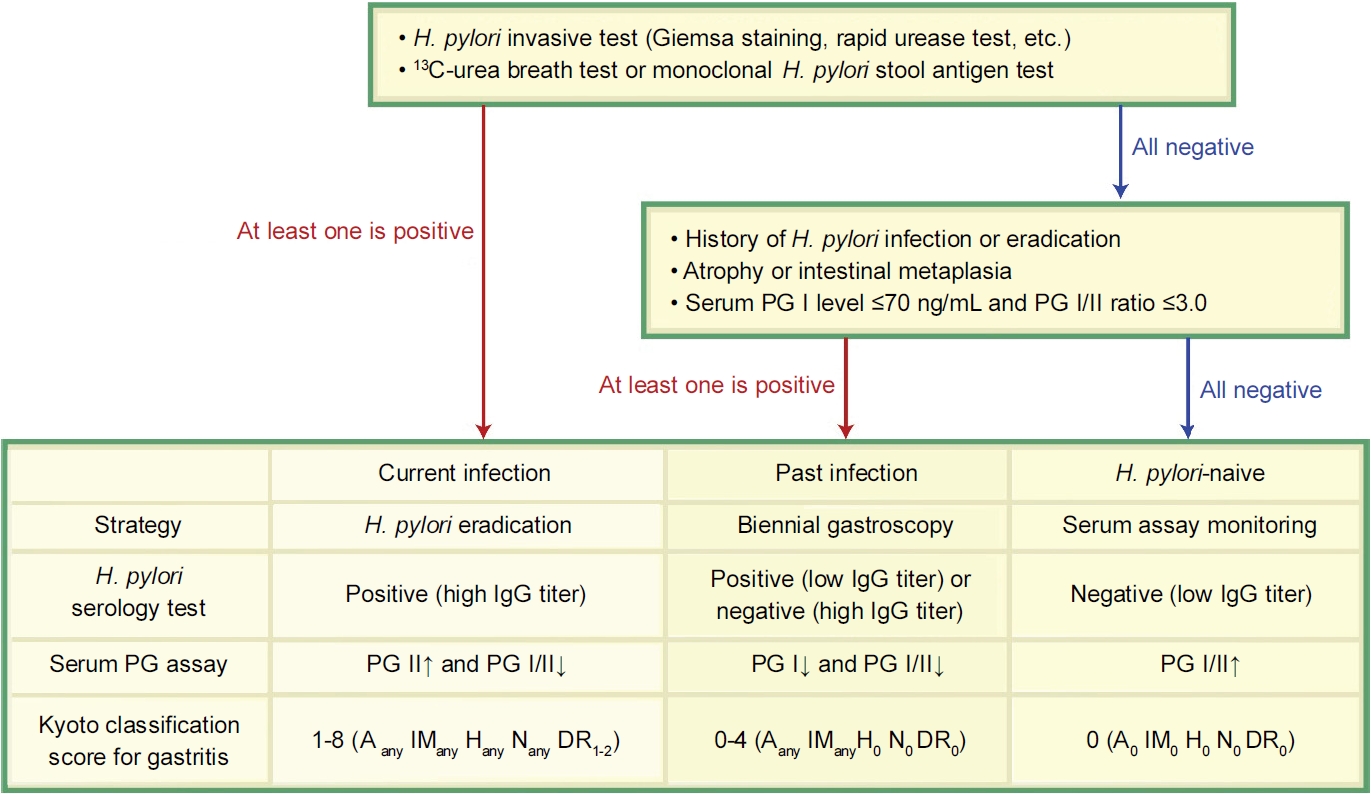
To diagnose H. pylori infection, serum assay findings should be interpreted together with gastroscopy findings of the background mucosa and other H. pylori tests. When current H. pylori infection is suspected, either a positive UBT, monoclonal H. pylori stool antigen test or invasive test finding is required for confirmation (Fig. 2). If there is an infection, primary prevention (H. pylori eradication) should be achieved before recommending secondary prevention (biennial endoscopic screening) for gastric cancer [10].
After eradication, confirmation should be done using UBT or a monoclonal-type stool antigen test because they show high specificities (UBT: 97.9~100%, stool test: 97.0~100%) and sensitivities (UBT: 97.7~100%, stool test: 96.0~100%) among all H. pylori tests [11]. Conversely, invasive H. pylori tests should be avoided because endoscopic biopsies often show false negative findings [12]. Although serum assays are not used for eradication confirmation, PG II levels and serology titers start to decrease within a few months after successful eradication [13]. Moreover, PG I/II ratios start to increase several months after eradication unless severe gastric corpus atrophy is present [14]. These changes are more profound in younger eradicated patients than in older patients with atrophy [15]. Furthermore, PG levels increase in renal failure patients and after the use of certain drugs, including aspirin and acid suppressants. Conversely, PG levels decrease after gastrectomy owing to the loss of chief cells. Altogether, it should be kept in mind that there is a wide variation in PG levels among individuals.
Past infection can be diagnosed if there is an eradication history, intestinal metaplasia, or atrophy (including gastric corpus atrophy as measured by a PG I/II ratio ≤3.0 and PG I level ≤70 ng/mL) (Fig. 2). The risk of gastric cancer is higher in eradicated patients than in H. pylori-naive individuals; hence, biennial gastroscopy is recommended. In a recent Korean study, gastroscopy decreased gastric cancer-related death, with a hazard ratio of 0.57 when screening endoscopy was performed within ≤23 months [16].
H. pylori-naive individuals show the lowest risk of gastric cancer among all infection statuses [17]. In their study, 1,378 (75.2%) of 1,833 Korean gastric cancer patients had current infection, 412 (22.5%) had a past infection, and 43 (2.3%) had no infection history. As summarized in Fig. 1, neuroendocrine tumors and other rare H. pylori-negative gastric cancers may occur in H. pylori-naive stomachs. Precancerous conditions for neuroendocrine tumors are autoimmune gastritis [18] and hypergastrinemia induced by a long-term intake of a potassium-competitive acid blocker (P-CAB) or proton pump inhibitor (PPI) [19]. Unlike histamine type-2 receptor antagonists, PPI and P-CAB induce hypersecretion of gastrin and PG [20]. Therefore, serum gastrin levels should be monitored when PPI or P-CAB is administered for a long time.
In summary, gastric cancer screening methods should vary according to H. pylori infection status because the risks and characteristics of gastric cancers differ among H. pylori-infected, -eradicated, and -naive individuals. The current strategy using biennial gastroscopy should be recommended only to individuals with an infection history. When there is an infection, H. pylori should be eradicated first, and confirmation should be followed using UBT or a monoclonal stool antigen test. Furthermore, monitoring serum gastrin levels would be helpful to H. pylori-naive subjects when administrating acid suppressants. To implement these different strategies, Korean endoscopists should be aware of serum assay and gastroscopy findings that indicate H. pylori-infected, -eradicated, and -naive stomachs. Additional training on diagnosing H. pylori infection status is required for all endoscopists engaged in gastric cancer screening.